Hysteroscopy involves visualization of uterine cavity for diagnostic or therapeutic purposes.
Diagnostic procedures are required :-
- To find the cause of abnormal uterine bleeding and obtain a biopsy
- To investigate cause of primary or secondary infertility
- In recurrent miscarriages
Therapeutic procedures are :-
- Removal of submucous fibroids
- Removal of polyps
- Resection of intrauterine septum
- Targeted biopsy
- Adhesiolysis of intrauterine synechiae
Hysteroscopic procedures require distension of the uterine cavity. The most common distending media that have been used are :-
- Carbon dioxide gas
- Glycine, Mannitol or sorbitol that are hypotonic
- Normal Saline, which is isotonic
Carbon dioxide is no longer used as distension medium as vision is obscured due to bleeding during the procedure. Hence fluid media are preferred. The equipment used for distension is called hysteromat or endomat. The maximum pressure should be 70-100 mm Hg or pressure just adequate to visualize uterine cavity. Resection of the endometrium or fibroids requires use of large diameter hysteroscopes with continuous flow of irrigating medium. They involve a working element with electrically active loop using monopolar current with non-electrolyte distending media like glycine or sorbitol. However, these solutions are hypotonic and utmost vigilance is required to prevent excessive absorption, which may cause life-threatening hyponatremia. Isotonic electrolyte containing fluids like normal saline cannot be used with monopolar energy as it leads to activation of ions and dispersal of electric current and hence reduce power density, which may be ineffective to destroy the tissue. Newer resectoscopes have been developed to use bipolar current and they are compatible with electrolyte containing distension media such as ringer lactate or normal saline. These solutions have reduced the incidence of hyponatremia considerably.
Anesthesia for Hysteroscopic procedures
Regional anesthesia either spinal or epidural is preferred over general anesthesia for early recognition of symptoms of fluid overload.
Short procedures like diagnostic hysteroscopy can be done under total intravenous anesthesia (TIVA).
General anesthesia is given if the patient is anxious or if laparoscopy may be done along with hysteroscopy where either laryngeal mask airway or endotracheal tube is inserted. Hysteroscopy may also be performed as an office procedure using miniature (1.9 mm) hysteroscope. Oral administration of NSAIDs should be done to reduce pain during procedure, opiates are not recommended. Intracervical and paracervical infiltration of local anesthetic can be done to alleviate vasovagal response during the procedure.
Complications of Hysteroscopy are
- Fluid overload or TURP like syndrome
- Air embolism
- Uterine perforation
Fluid overload
Fluid deficit is defined as difference between the volume of irrigating fluid that goes inside the uterine cavity and that flushes out of the uterine cavity during the procedure.
Fluid deficit of 1000 ml results in fluid overload while using hypotonic solution like glycine. Fluid deficit of 2500 ml while using isotonic solution like normal saline may cause fluid overload in a healthy woman of reproductive age group. However, for women with cardiorespiratory compromise or renal impairment, threshold should be reduced to 750 ml for hypotonic solution and 1500 ml for isotonic solution.
Absorption of distension medium from open sinuses of the uterine cavity can cause fluid overload. It can occur with both isotonic and hypotonic solutions; however, incidence is higher with hypotonic solutions.
Factors, which lead to fluid, overload are :-
High intrauterine distension pressure, duration of procedure, depth of myometrial penetration, size of myoma and volume of medium used.
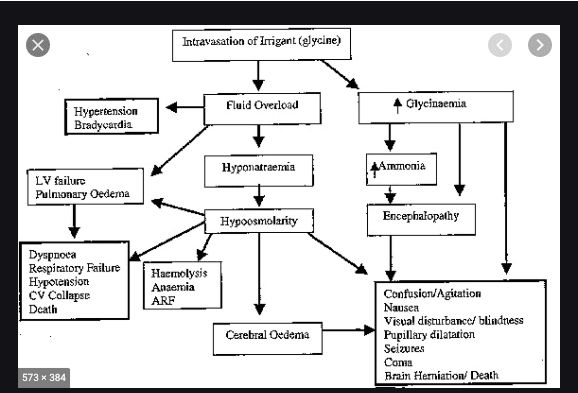
Signs and symptoms of fluid overload are due to hyponatremia, which is common with glycine or any hypotonic medium. Patient will have
- Nausea, vomiting
- Confusion, disorientation
- Focal weakness, convulsions
- Pulmonary edema and cardiac failure
- Coma, respiratory arrest, brainstem herniation, death
Input and output should be meticulously calculated using calibrated drapes and reservoirs and must be assessed at every 10-minute interval. A closed loop system should be employed for exact estimation of input and output of the distension medium. A decrease in serum sodium of 10mmol/L corresponds to 1000 ml of fluid absorbed if the solution is 1.5% glycine.
Management of suspected hypervolaemic hyponatraemia due to fluid overload
Moderate fluid overload causes hypervolaemia and dilutional hyponatraemia. If serum Na+ concentration falls below 120 mmol/L, symptoms develop. Patient complains of headache, nausea, vomiting, weakness. If intravasation continues, water moves into intracellular and interstitial space leading to brain edema and rise in intracranial pressure. Patient may have symptoms like agitation, confusion, nausea, vomiting, headache and visual disturbances. If continued can lead to brain stem herniation, coma and death.
Asymptomatic hyponatraemia can be treated with fluid restriction and frusemide.
Symptomatic hyponatraemia requires multidisciplinary approach and high dependency care. 100ml bolus of 3% saline over 10 min to be repeated 3 times followed by IV infusion of 3% hypertonic saline 1-2 mmol/L/h is indicated. The target is to increase serum sodium 6 mmol/L over 24 hours until 130 mmol/L is achieved. Rapid correction of hyponatremia may cause pontine myelinolysis or osmotic demyelination syndrome. After recovery from hyponatremai, a biphasic reaction occurs and patient suffers from swallowing difficulty, gait changes and other neurological symptoms.
| Acute hypervolamic hyponatraemia | Management |
| Asymptomatic hyponatraemia (Na+ >120 mm0l/L | Fluid restriction<1L/day and 40 mg frusemide |
| Symptomatic hypoosmolar (Na+ <120 mmol/L | Hypertonic saline (3%) (1L=513 mmol, Normal saline 1L =154mmol) Supplemental oxygen, indwelling urinary catheter, high dependency unit, multidisciplinary involvement |
Air or gas embolism during hysteroscopy
Air or gas embolism is rare but can occur during hysteroscopic procedure. Air can enter the uterine cavity if the tube is not primed with fluid or appearance of bubbles in the solution. If the patient develops sudden desaturation, air embolism should be suspected.
Tips and tricks to reduce fluid absorption
- Use of GnRh agonist before resection of myoma, which can reduce the volume of fibroid
- Intracervical injection of dilute vasopressin reduces absorption of fluid.
- 3. Intrauterine pressure should be kept below mean arterial pressure. A pressure between 70-100 mm Hg is considered safe.
- Use of automated fluid administering systems which maintain a constant pressure and accurate calculation of fluid deficit.
References:-
- 2013 AAGL Practice Report: practical Guidelines for the Management of hysteroscopic distension media. J Minim Invasive Gynecol 20:137–148.
- Propst A, Liberman RF, Harlow BL, Ginsburg ES (2000) Complications of hysteroscopic surgery: predicting patients at risk. Obstet Gynecol 96:517–520
- Aydeniz B, Gruber IV, Schauf B, Kurek R, Meyer A, Wallwiener D (2002) A multicenter survey of complications associated with 21676 operative hysteroscopies. Eur J Obstet Gynecol Reprod Biol 104:160–164
- aschopoulos M, Polyzos NP, Lavasidis LG, Vrekoussis T, Dalkalitsis N, Paraskevaidis E (2006) Safety issues of hysteroscop- ic surgery. Ann N Y Acad Sci 1092:229–234
- Varol N, Maher P, Vancaillie T, Cooper M, Carter J, Kwok A, Reid G (2002) A literature review and update on the prevention and management of fluid overload in endometrial resection and hyster- oscopic surgery. Gynaecol Endosc 11(1):19–26
- Cooper NAM, Smith P, Khan KS, Clark TJ.Analgesia and conscious sedation for pain control during outpatient hysteroscopy: a systematic review and meta-analysis; 2009. Personal communication.
- Cicinelli E, Didonna T,Ambrosi G, Schönauer LM, Fiore G, Matteo MG.Topical anaesthesia for diagnostic hysteroscopy and endometrial biopsy in postmenopausal women: a randomised placebo-controlled double-blind study. Br J Obstet Gynaecol 1997; 104:316–9.
- Lau WC,Tam WH, Lo WK,Yuen PM.A randomized double- blind placebo-controlled trial of transcervical intrauterine local anaesthesia in outpatient hysteroscopy. BJOG 2000; 107:610–3.
By Dr. Manisha Shembekar
Consultant Anaesthesia





