
Pulmonary hypertension is a major reason for elevated perioperative morbidity and mortality, even in non-cardiac surgical procedures. All specialty units involved in treatment should play a role. After selecting each of the suitable individual anaesthetic and surgical procedures, intraoperative management should focus on avoiding all circumstances that could contribute to exacerbating pulmonary hypertension (hypoxemia, hypercapnia, acidosis, hypothermia, hypervolemia, and insufficient anaesthesia and analgesia).
Stress, pain, ventilation, and surgery-related inflammation can increase pressure and resistance within the pulmonary arteries and cause right-sided heart failure. A number of independent factors lead to an increased perioperative risk for patients with pulmonary hypertension viz. heart failure of NYHA class II or higher, a history of pulmonary embolism, high-risk surgery (e.g., thoracic or major abdominal surgery), and an anaesthesia duration of more than 3 hours. The literature reports a perioperative mortality of 7–24%, with the highest risk for pregnant women and patients undergoing emergency interventions. The PH patients have a significantly increased risk for hemodynamic instability, heart failure, postoperative sepsis, and respiratory failure, significantly prolonged postoperative ventilation, a longer intensive care stay and more frequent readmissions in first 30 days after surgery.
Definition and Pathophysiology of Pulmonary Hypertension
Pulmonary hypertension comprises a number of diseases, all of which have the common symptom of increased pressure in the pulmonary arteries.
PH is defined as mean PAP > 24mmHg at rest. Values of mean PAP 20mmHg or more BUT ≤ 24 mmHg are referred to as borderline PH. Mean pulmonary artery pressure in healthy persons is 14 ± 3mmHg. PH may be divided into precapillary and post capillary PH.
Hemodynamic characteristics in patients with Pulmonary Hypertension
The pulmonary circulation is characterized by high flow, low pressure, and low resistance.
PH can be classified as precapillary if PAWP is 15 mm Hg or lower or as post capillary if PAWP is higher than 15 mm Hg.
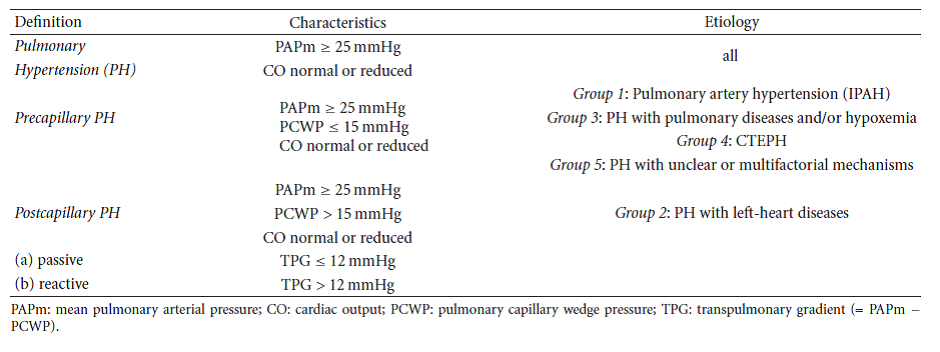
Fig. 1 –
During exercise– mPAP is dependent on the exercise level and age.
With mild exercise-mPAP is 19.4 ± 4.8 mm Hg in subjects younger than 50 years versus 29.4 ± 8.4 mm Hg in subjects 50 years or older.
Exercise mPAP is related to age and frequently exceeds 30 mm Hg, especially in elderly individuals, which makes it difficult to define normal mPAP values during exercise.
Given these circumstances, the diagnosis of exercise-induced PH was abandoned in 2008 because of insufficient evidence.
The normal pulmonary vascular bed offers less than 10% of the resistance to flow than does the systemic bed and can be approximated as the ratio of the drop in pressure (in mm Hg) to mean flow (in liter/min).
PVR can be calculated as the ratio (mPAP − PAWP)/CO, whereas total pulmonary resistance (TPR) corresponds to the ratio mPAP/CO. The ratio can be multiplied by 80 to express the results in dyne-sec • cm −5 or be expressed in mm Hg/liter/min, which is referred to as a Wood unit.
The calculated PVR in normal adults is 67 ± 23 dyne-sec • cm −5 (or 1 Wood unit).
The physiologic range of PVR and TPR and the impact of exercise, age, and posture have been a matter of debate for many years
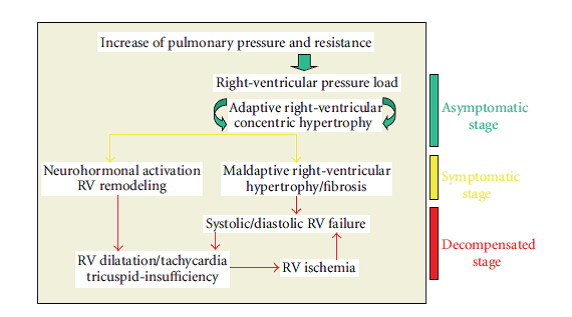
Fig. 2 – Development of right-ventricular failure in patients with pulmonary hypertension.
Preoperative Preparation and Diagnostics: A multidisciplinary Task
Given that pulmonary hypertension affects several organ systems simultaneously (lung, heart, and vascular system), preparations for the surgical procedure should be considered as the joint task of anaesthesia, surgery, pulmonology, and cardiology.
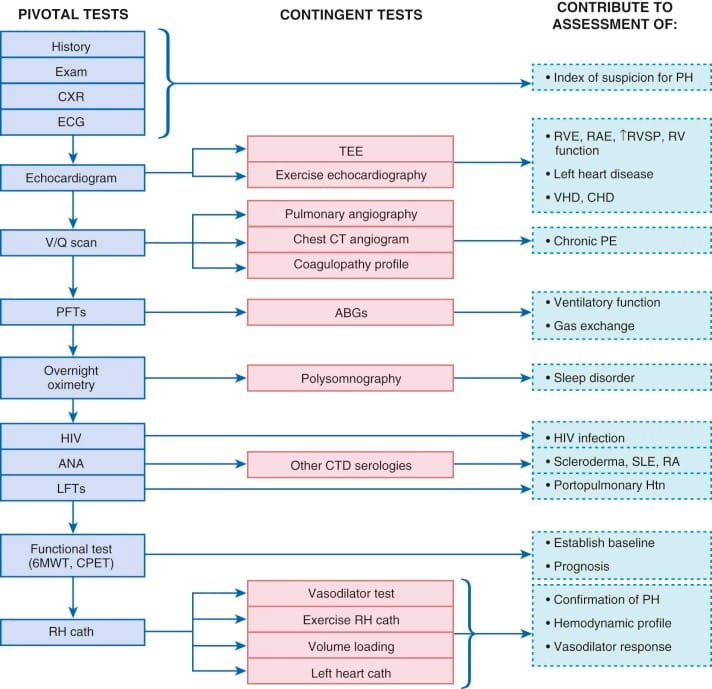
Fig. 3 –
- Clinical Examination.
The clinical symptoms of pulmonary hypertension are largely nonspecific and easily overlooked or misinterpreted in the early disease stages .The most common but, unfortunately, very unspecific symptom is stress-induced dyspnea.
Clinical findings in patients with pulmonary hypertension
(a) Dyspnea (during stress/at rest)/cyanosis
(b) Fatigue
(c) Dizziness
(d) Syncope
(e) Thoracic pain
(f) Palpitations
(g) Orthopnea
(h) Cough
(i) Croakiness
(j) Abdominal tension
(k) Peripheral Edema/Ascites
(l) Hepatomegaly
Thoracic X-Ray. Characteristic findings for pulmonary hypertension include right-ventricular hypertrophy, dilation of the central pulmonary arteries, and vascular rarefaction in the peripheral pulmonary parenchyma
ECG
(i) Sinus tachycardia
(ii) Vertical/right type
(iii) Positive Sokolow-Lyon index for right-ventricular hypertrophy
(iv) p-pulmonalis
(v) SI/SII/SIII-Type and SI/QIII-Type
(vi) Incomplete or complete right bundle branch block
(vii) Right-ventricular repolarization disorder

Fig. 4 –
Echocardiography. Echocardiography is currently the non-invasive method with the highest sensitivity and specificity for diagnosing PH.
OTHER TESTS:
-PFT
-TEE
-Spirometry
-right heart catheterization
TREATMENT
Optimization of Primary Disease Therapy.
At the time of surgery, the patient should ideally have been in a stable condition for an extended period of time. If the pulmonary hypertension was discovered immediately prior to urgent surgery that could not be postponed, Fox et al. recommended starting treatment with sildenafil (50–100 mg/day) and L-arginine (15 g/day) as early as possible.
Intraoperative Monitoring.
Recommendation for patients with PH.
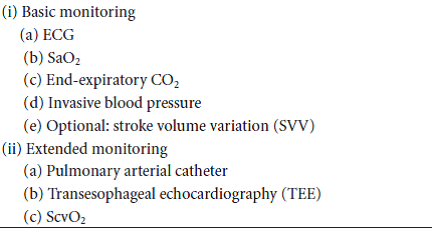
Fig. 5
Selection of the Anaesthetic Technique
All standard anaesthetic techniques can, in principle, be applied to patients with pulmonary hypertension.
Regional anaesthetic techniques offer the advantage of not impairing spontaneous breathing and of avoiding elevated pulmonary pressure, which is induced by mechanical ventilation. In addition, techniques of continuous regional anaesthesia can be used for postoperative analgesic therapy. In general, continuous techniques should be preferred to bolus administration—especially for procedures in the vicinity of the spinal cord—in order to avoid uncontrolled drops in blood pressure, which can endanger myocardial perfusion.
During induction of epidural analgesia, administration and dosing of local anaesthetics should be performed carefully and fractionated in order to avoid significant decrease in systemic vascular resistance, reduction of coronary perfusion, and right-heart failure. Due to this risk, spinal anaesthesia with bolus technique should be avoided and also replaced by a catheter technique to avoid any significant effects on hemodynamic. Thoracic epidural anaesthesia does not have any significant influence on oxygenation and pulmonary vascular tension, however, a high ratio (TH1-TH4) can cause sympathetic blockade and therefore a decrease in myocardial inotropy and chronotropy.
Plexus catheters or nerve catheters (sciatic or femoral nerve) are recommended for surgical procedures involving the extremities in particular, as they do not affect hemodynamics.
Techniques in the vicinity of the spinal cord can be applied both in hernia surgery and in urological or gynaecological interventions. In abdominal and thoracic surgery in particular, it is advisable to combine general and thoracic epidural anaesthesia in order to reduce intraoperative consumption of anaesthetic agents and to avoid high doses of systemic opioid analgesics in the postoperative phase.
The main advantages of general anaesthesia are safe oxygenation and uncomplicated airway management. When the patient is intubated during anaesthesia, inhalants for selective pulmonary vasodilation can easily be administered through the breathing gas. The combination of anaesthetic-agent-induced systemic vasodilation and mechanical ventilation can lead to a significant drop in mean arterial pressure, which has the potential to reduce coronary perfusion pressure and critically affect right-ventricular contractility.
All standard induction agents (recommended doses: thiopental 2–5 mg/kg, propofol 1-2mg/kg, and etomidate 0.2–0.4mg/kg KG) can, in principle, be used in combination with opioids (recommended doses: fentanyl 5–10 μg/kg KG and sufentanil 0.5– 1 μg/kg KG), as they have no influence on pulmonary vascular resistance and oxygenation [50–52]. Histamine-releasing relaxants (atracurium, mivacurium) should be avoided for patients with pulmonary hypertension, as they may further increase pulmonary resistance.
Intraoperative Management and Treatment of Intraoperative PA Pressure Elevation.
The most important requirement for intraoperative management and maintenance of anesthesia is to avoid anything that could increase right-ventricular afterload or decrease contractility of the right ventricle, as both factors will ultimately lead to ischemia and right-sided heart failure.
Intraoperative “basic treatment” to avoid an increase of pulmonary arterial pressure
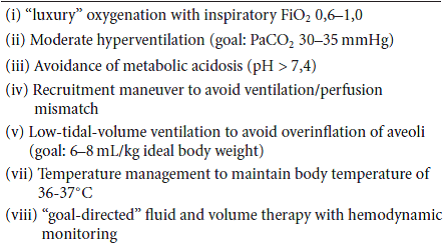
Fig. 6
Specific interventions for therapy of intra- and/or postoperative increase of pulmonary arterial pressure
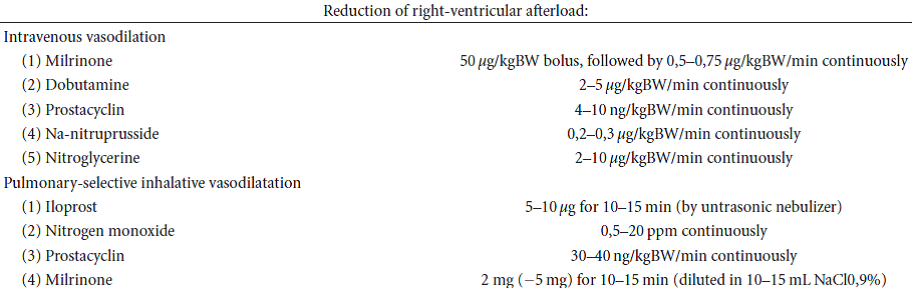
Fig. 7
Postoperative Recovery and Analgesic Therapy.
Patients with pulmonary hypertension are at risk of developing elevated pulmonary pressure and right-sided heart failure not only during the perioperative phase itself, but also in the postoperative course. These patients should therefore be placed under intense postoperative monitoring for a period appropriate to the degree of surgical trauma; the target monitoring time should be between 24 hours for small interventions and several days for major procedures (abdominal and thoracic surgery, major urological interventions).
CONCLUSION
Perioperative management of patients with pulmonary hypertension presents an interdisciplinary challenge that requires the adequate involvement of anaesthetists, surgeons, pulmonologists, and cardiologists alike.





