
Prof and Head, Chest & TB,
IGGMC, Nagpur
We have heard and often talked about pink puffers and blue bloaters which are the characteristic presentation of patients of COPD . Chronic obstructive pulmonary disease (COPD) represents an important and increasing burden throughout the world. Classically, COPD has been considered a respiratory condition only, mainly caused by tobacco smoking. However now it is known and established that COPD has important manifestations beyond the lungs, the so-called systemic effects. Low-grade, chronic systemic inflammation is one of the key mechanisms underlying these systemic effects. Because these extra-pulmonary manifestations of COPD are common and/or may have significant implications for the patient wellbeing and prognosis, they also warrant systematic screening and appropriate management in order to provide optimal medical care.
DEFINITION
Chronic Obstructive Pulmonary Disease (COPD) is a common preventable and treatable disease, is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases.(According to recent Global Initiative for Chronic Obstructive Lung Disease (GOLD) Guidelines) This definition does not use the terms chronic bronchitis and emphysema and excludes asthma (reversible airflow limitation
Exacerbations and comorbidities contribute to the overall severity in individual patients 1. Spirometry is required to make a clinical diagnosis of COPD; the presence of a post-bronchodilator FEV1/FVC < 0.70 confirms the presence of persistent airflow limitation 2 and thus of COPD.
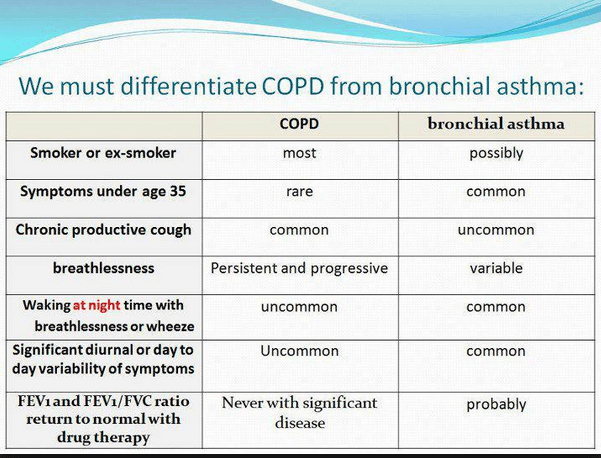
In contrast to bronchial asthma where post bronchodilator spirometry has an improvement of 200ml or 12% in FEV1and with diurnal variation in PEFR value.
However some patients of COPD do show reversibility and in some patients there is always an overlap in presentation as shown in the diagram.

Epidemiology
Worldwide, the most commonly encountered risk factor for COPD is tobacco smoking.
Nonsmokers may also develop COPD.The genetic risk factor that is best documented is a severe hereditary deficiency of alpha-1 antitrypsin 7. It provides a model for how other genetic risk factors are thought to contribute to COPD.COPD risk is related to the total burden of inhaled particles a person encounters over their lifetime:
- Tobacco smoke 8-9, including cigarette, pipe, cigar, and other types of tobacco smoking popular in many countries, as well as environmental tobacco smoke (ETS)
- Occupational dusts and chemicals 10-13 (vapors, irritants, and fumes) when the exposures are sufficiently intense or prolonged
- Indoor air pollution 14-20 from biomass fuel used for cooking and heating in poorly
Vented dwellings, a risk factor that particularly affects women in developing
countries - Outdoor air pollution also contributes to the lungs’ total burden of inhaled particles.
Although it appears to have a relatively small effect in causing COPD - 5. In addition, any factor that affects lung growth during gestation and childhood 21-23
(low birth weight, respiratory infections, etc.) has the potential to increase an
individual’s risk of developing COPD.
PATHOLOGY, PATHOGENESIS AND PATHOPHYSIOLOGY
Inhaled cigarette smoke and other noxious particles such as smoke from biomass fuels cause lung inflammation, a normal response that appears to be modified in patients who develop COPD.This chronic inflammatory response may induces parenchymal tissue destruction (resulting in emphysema), and disrupt normal repair and defense mechanisms(resulting in small airway fibrosis).These pathological changes lead to air trapping and progressive airflow limitation 24.
Pathology
The pathological changes include chronic inflammation, with increased numbers of specific inflammatory cell types in different parts of the lung, and structural changes resulting from repeated injury and repair. Pathological changes characteristic of COPD are found in the airways, lung parenchyma, and pulmonary vasculature 25. In general, the inflammatory and structural changes in the airways increase with disease severity and persist on smoking
Pathogenesis
The inflammation in the respiratory tract of COPD patients appears to be a modification of the inflammatory response of the respiratory tract to chronic irritants such as cigarette smoke.
The mechanisms for this amplified inflammation are not yet understood but may be genetically determined. Patients can clearly develop COPD without smoking, but the nature of the inflammatory response in these patients is unknown. Oxidative stress and an excess of proteinases in the lung further modify lung inflammation. Together, these mechanisms lead to the characteristic pathological changes in COPD.Lung inflammation persists after smoking cessation through unknown mechanisms, although autoantigens and persistent microorganisms may play a role
Oxidative Stress
Oxidative stress may be an important amplifying mechanism in COPD 26.Biomarkers of oxidative stress (e.g., hydrogen peroxide, 8-isoprostane) are increased in the exhaled breath condensate, sputum, and systemic circulation of COPD patients. Oxidative stress is further increased in exacerbations. Oxidants are generated by cigarette smoke and other inhaled particulates,and released from activated inflammatory cells such as macrophages and neutrophils 27.There may also be a reduction in endogenous antioxidants in COPD patients as a result of reduction in a transcription factor called Nrf2 that regulates many antioxidant genes.
Protease-Antiprotease Imbalance
There is compelling evidence for an imbalance in the lungs of COPD patients between proteases that break down connective tissue components and antiproteases that protect against this. Several proteases,derived from inflammatory cells and epithelial cells, are increased in COPD patients. There is increasing evidence that they may interact with each other. Protease-mediated destruction of elastin, a major connective tissue component in lung parenchyma,is believed to be an important feature of emphysema and is likely to be irreversible.
Inflammatory Cells
COPD is characterized by a specific pattern of inflammation involving increased numbers of
CD8+ (cytotoxic) Tc1 lymphocytes present only in smokers that develop the disease,these cells, together with neutrophils and macrophages, release inflammatory mediators and enzymes and interact with structural cells in the airways, lung parenchyma and pulmonary Vasculature.
Inflammatory Mediators
The wide variety of inflammatory mediators that have been shown to be increased in COPD patients 28 attract inflammatory cells from the circulation(chemotactic factors), amplify the inflammatory process (proinflammatory cytokines), and induce structural changes (growth factors). Although both COPD and asthma are associated with chronic inflammation of the respiratory tract, there are differences in the inflammatory cells and mediators involved in the two diseases,which in turn account for differences in physiological effects, symptoms, and response to therapy 29.Some patients with COPD have features consistent with asthma and may have a mixed inflammatory pattern with increased eosinophils.
Pathophysiology
Airflow Limitation and Air Trapping
The extent of inflammation, fibrosis, and luminal exudates in small airways is correlated with the reduction in FEV1and FEV1/FVC ratio, and probably with the accelerated decline in FEV1 characteristic of COPD 30. Inflammation and narrowing of peripheral airways leads to decreased FEV1.Parenchymal destruction due to emphysema also contributes to airflow limitation and leads to decreased gas transfer.This peripheral airway obstruction progressively traps air during expiration,resulting in hyperinflation. Although emphysema is more associated with gas exchange abnormalities than with reduced FEV1,it does contribute to gas trapping during expiration. This is especially so as alveolar attachments to small airways are destroyed when the disease becomes more severe. Hyperinflation reduces inspiratory capacity such that functional residual capacity increases, particularly during exercise (dynamic hyperinflation), resulting in increased dyspnea and limitation of exercise capacity.These factors contribute to impairment of the intrinsic contractile properties of respiratory muscles; this results in upregulation of local pro-inflammatory cytokines. It is thought that hyperinflation develops early in the disease and is the main mechanism for exertional dyspnea 31
Bronchodilators acting on peripheral airways reduce air trapping, thereby reducing lung volumes and improving symptoms and exercise capacity.
Gas Exchange Abnormalities
Gas exchange abnormalities result in hypoxemia and hypercapnia and have several mechanisms in COPD. In general, gas transfer for oxygen and carbon dioxide worsens as the disease progresses. Reduced ventilation may also be due to reduced ventilatory drive. This may lead to carbon dioxide retention when it is combined with reduced ventilation due to a high work of breathing because of severe obstruction and hyperinflation coupled with ventilatory muscle impairment. The abnormalities in alveolar ventilation and a reduced pulmonary vascular bed further worsen the V A/Q abnormalities
Mucus Hypersecretion
Mucus hypersecretion, resulting in a chronic productive cough, is a feature of chronic bronchitis and is not necessarily associated with airflow limitation.Conversely, not all patients with COPD have symptomatic mucus hypersecretion. When present, it is due to an increased number of goblet cells and enlarged submucosal glands in response to chronic airway irritation by cigarette smoke and other noxious agents. Several mediators and proteases stimulate mucus hypersecretion and many of them exert their effects through the activation of epidermal growth factor receptor (EGFR)
Pulmonary Hypertension
Pulmonary hypertension may develop late in the course of COPD and is due mainly to hypoxic vasoconstriction of small pulmonary arteries, eventually resulting in structural changes that include intimal hyperplasia and later smooth muscle hypertrophy/hyperplasia.
There is an inflammatory response in vessels similar to that seen in the airways and evidence of endothelial cell dysfunction. The loss of the pulmonary capillary bed in emphysema may also contribute to increased pressure in the pulmonary circulation. Progressive pulmonary hypertension may lead to right ventricular hypertrophy and eventually to right-side cardiac failure.
DIAGNOSIS
A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease (Table 1).
Key Indicators for Considering a Diagnosis of COPD
Consider COPD,and perform spirometry,if any of these indicators are present in an individual over age 40.These indicators are not diagnostic themselves,But the presence of multiple key indicators increases the probability of a diagnosis of COPD.Spirometry Is required to establish a diagnosis of COPD.
| Dyspnea that is: | Progressive (worsens over time). |
| Chronic cough: | May be intermittent and may be unproductive. |
| Chronic sputum production: | Any pattern of chronic sputum production may indicate COPD. |
| History of exposure to risk factors: | Tobacco smoke (including popular local preparations). Smoke from home cooking and heating fuels. Occupational dusts and chemicals. |
| Family history of COPD |
Spirometry is required to make a clinical diagnosis of COPD; the presence of a postbronchodilator FEV1/FVC < 0.70 confirms the presence of persistent airflow limitation and thus of COPD.
Differential Diagnosis:
A major differential diagnosis is asthma. In some patients with chronic asthma, a clear distinction from COPD is not possible using current imaging and physiological testing techniques. In these patients,current management is similar to that of asthma. Other potential diagnoses are usually easier to distinguish from COPD. COPD and its Differential Diagnoses
| 1. COPD | Onset in mid-life. Symptoms slowly progressive. History of tobacco smoking or exposure to other types of smoke. |
| 2. Asthma | Onset early in life (often childhood). Symptoms vary widely from day to day. Symptoms worse at night/early morning. Allergy, rhinitis, and/or eczema also present. Family history of asthma. |
| 3. Congestive Heart Failure | Chest X-ray shows dilated heart, pulmonary edema. Pulmonary function tests indicate volume restriction,not airflow limitation. |
| 4. Bronchiectasis | Large volumes of purulent sputum. Commonly associated with bacterial infection. Chest X-ray/CT shows bronchial dilation, bronchial wall thickening. |
| 5. Tuberculosis | Onset all ages. Chest X-ray shows lung infiltrate. Microbiological confirmation. High local prevalence of tuberculosis. |
| 6. Obliterative Bronchiolitis | Onset at younger age, nonsmokers. May have history of rheumatoid arthritis or acute fume exposure. Seen after lung or bone marrow transplantation. CT on expiration shows hypodense areas. |
| 7. Diffuse Panbronchiolitis | Predominantly seen in patients of Asian descent. Most patients are male and nonsmokers. Almost all have chronic sinusitis. Chest X-ray and HRCT show diffuse small centrilobular nodular opacities and hyperinflation. |
ASSESSMENT OF COPD
The goals of COPD assessment are to determine the severity of the disease, its impact on patient’s health status, and the risk of future events (exacerbations,hospital admissions, death) in order to guide therapy. Assess the following aspects of the disease separately:
- Symptoms
- Degree of airflow limitation (using spirometry)
- Risk of exacerbations
- Comorbidities
Assess Symptoms
Validated questionnaires such as the COPD Assessment Test (CAT) or the Modified British Medical Research Council (mMRC) breathlessness scale should be used to assess symptoms.
Assess Degree of Airflow Limitation Using Spirometry:
Classification of Severity of Airflow Limitation in COPD | ||
| GOLD 1: | Mild | FEV1≥ 80% predicted |
| GOLD 2: | Moderat | 50% ≤ FEV1< 80% predicted |
| GOLD 3: | Severe | 30% ≤ FEV1< 50% predicted |
| GOLD 4: | Very Severe | FEV1< 30% predicted |
Assess Risk of Exacerbations
An exacerbation of COPD is defined as an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication.The best predictor of having frequent exacerbations (2 or more per year) is a history of previous treated events; the risk of exacerbations also increases as airflow limitation worsens.
Assess Comorbidities
Cardiovascular diseases, osteoporosis, depression and anxiety, skeletal muscle dysfunction, metabolic syndrome, and lung cancer among other diseases occur frequently in COPD patients. These comorbid conditions may influence mortality and hospitalizations, and should be looked for routinely and treated appropriately.
Additional Investigations
The following additional investigations may be considered as part of the diagnosis and assessment of COPD:
1. Imaging
A chest X-ray is not useful to establish a diagnosis in COPD, but it is valuable in excluding alternative diagnoses and establishing the presence of significant comorbidities such as concomitant respiratory (pulmonary fibrosis, bronchiectasis, pleural diseases), skeletal (e.g., kyphoscoliosis), and cardiac diseases (e.g., cardiomegaly). Radiological changes associated with COPD include signs of lung hyperinflation (flattened diaphragm on the lateral chest film, and an increase in the volume of the retrosternal air space), hyperlucency of the lungs, and rapid tapering of the vascular markings.
Computed tomography (CT) of the chest- is not routinely recommended. However, when there is doubt about the diagnosis of COPD, CT scanning might help in the differential diagnosis where concomitant diseases are present. In addition, if a surgical procedure such as lung volume reduction is contemplated, a chest CT scan is necessary since the distribution of emphysema is one of the most important determinants of surgical suitability.
2. Lung Volumes and Diffusing Capacity
COPD patients exhibit gas trapping (a rise in residual volume) from early in the disease, and as airflow limitation worsens static hyperinflation (an increase in total lung capacity) occurs. These changes can be documented by body plethysmography,or less accurately by helium dilution lung volume measurement. These measurements help characterize the severity of COPD but are not essential to patient management.
Measurement of diffusing capacity (DLCO) provides information on the functional impact of emphysema in COPD and is often helpful in patients with breathlessness that may seem out of proportion with the degree of airflow limitation.
3. Oximetry and Arterial Blood Gas Measurement
Pulse oximetry can be used to evaluate a patient’s oxygen saturation and need for supplemental oxygen therapy. Pulse oximetry should be used to assess all stable patients with FEV1< 35% predicted or with clinical signs suggestive of respiratory failure or right heart failure. If peripheral saturation is < 92% arterial blood gases should be assessed.
4. Alpha-1 Antitrypsin Deficiency Screening
The World Health Organization recommends that COPD patients from areas with a particularly high prevalence of alpha-1 antitrypsin deficiency should be screened for this genetic disorder.However, the typical patient tends to present at a younger age (< 45 years) with lower lobe emphysema. Family members can be identified and family screening is useful for appropriate counseling. A serum concentration of alpha-1 antitrypsin below 15-20% of the normal value is highly suggestive of homozygous alpha-1 antitrypsin deficiency.
5. Exercise Testing
Objectively measured exercise impairment, assessed by a reduction in self-paced walking distance or during incremental exercise testing in a laboratory, is a powerful indicator of health status impairment and predictor of prognosis.Walking tests can be useful for assessing disability and are used to assess the effectiveness of pulmonary rehabilitation. Both the paced shuttle walk tests and the unpaced 6-minute walk test can be used.Laboratory testing using cycle or treadmill ergometry can identify co-existing or alternative conditions, e.g.,cardiac diagnoses. Monitoring of physical activity may be more relevant regarding prognosis than evaluating exercise capacity.This can be done using accelerometers or multisensor instruments.
| Patient | Characteristic | SpirometricClassification | ExacerbationsPer year | mMRC | CAT |
| A | Low risk Less symptoms | GOLD 1-2 | < Or = 1 | 0 – 1 | < 10 |
| B | Low risk More | GOLD 1-2 | < Or = 1 | > Or = 2 | > Or = 10 |
| C | High risk Less symptoms | GOLD 3-4 | > Or = 2 | 0 – 1 | < 10 |
| D | High risk More symptoms | GOLD 3-4 | > Or = 2 | > Or = 2 | > Or = 10 |
THERAPEUTIC OPTIONS
- Smoking cessation – has the greatest capacity to influence the natural history of COPD.
Counselling delivered by physicians & others significantly increases quit rates over self initiated strategies.Nicotine replacement therapy (nicotine gum,inhaler,nasal spray, transdermal patch,sublingual tablet or lozenges) as well as pharmacotherapy with,bupropion nortryptiline or verinicline reliably increases long term smoking absteinance rates. - Smoking prevention – Encourage tobacco control programs with clear,consistent & repeated Non smoking messages.Work with govt to pass legislationsd to establish smoke free schools,public facilities & work enviournment.
- Occupational exposure – emphasize primary prevention which is best achieved by elimination or reduction of exposures of various substances in work place.Secondary prevention,achieved through surveillance & early detection is also important.
- Indoor & outdoor Air pollution – Implement measures to reduce or avoid indooa air pollution from burning biomass fuels for cooking & heating in poorly ventilated areas.Advise patients to avoid vigorous exercise outdoors during pollution episodes.
- Physical activity – All COPD Patients benefit from regular physical activity & should be encouraged to remain active.
PHARMACOTHERAPY FOR STABLE COPD
Pharmacotherapy is used to reduce symptoms,reduce the frequency,severity of exacerbations & improve health status & exercise tolerance.Each treatment regimen needs to patient specific
- Bronchodilators-These are Important medications to control symptom management in COPD.
Inhaled therapy is preferred, Choice between beta2 agonists,anticholinergics,theophylline or combination therapy depends on availability & each patients individual response in terms of symptom relief & side effects. Prescibed on an as-needed or on a regular basis to prevent or reduce symptoms
Long acting inhaled bronchodilators are convenient & more effective at producing maintained symptom relief than short acting. Long acting inhaled bronchodilators also reduce exacerbations & related hospitalizations & improve symtoms & health status. Combination bronchodilators of different classewsmay improve efficacy & decrease risk of side effects compared to increasing the dose of single bronchodilator. - Inhaled steroids– In COPD patients, regular treatment with inhaled steroids improve symptoms,lung function & quality of life & reduce frequency of exacerbations .Withdrawl from treatment with inhaled steroids may lead to exacerbations in some patients .Long term monotherapy with inhaled steroids is not recommended.
- Combination Inhaled steroids/Bronchodilator therapy-An inhaled steroid combined with LABA is more effective than either individual component in improving lung function & health status & reducing exacerbations in patients with moderate to severe COPD.Addition of LABA/inhaled steroids to tiotropium appears to provide additional benefits.
- Oral steroids– Long term treatment with oral steroids is not recommended.
- Phosphodieterase-4 inhibitors- In GOLD-3 & GOLD-4 patients with history of exacerbations & chronic bronchitis, the phosphodieterase-4 inhibitor reduces exacerbations treated with oral steroids.These effects are also seen when added to long acting bronchodilators.
- Methylxanthines– are less effective & less well tolerated than inhaled long acting bronchodilators are not recommended if those drugs are available & affordable.Addition of theophylline to salmeterol produces greater increase in FEV1 & relief of breathlessness than salmeterol alone.low dose theophylline rduces exacerbations but doesnot improve lung functions.
- Other pharmacological treatments
- Vaccines- Influenza vaccine can reduce serious illness & death in COPD patients.Vaccines containing killed or live inactivated viruses are recommended & should be given once each year.Pneumococcal vaccine is recommended for COPD patients 65 yrs & older and has been shown to reduce pneumonia in those under 65 with severe COPD.
- Alpha1 antitrypsin augmentation therapy-recommended only in patients with Alpha1 antitrypsin therapy.
- Antibiotics-Not recommended except for treatment of infectious exacerbations & other bacterial infections.
- Mucolytic Agents-Patients with viscous sputum may benefit from mucolytics but overall benefits are very small.
OTHER TREATMENTS
- Rehabilitation-Patients at all stages of COPD benefit from exercise training programs with improvement in exercise tolerance& symptoms of dyspnea & fatigue. The minimum length of an effective program is 6 weeks;the longer the program continues,the more effective the results. Exercise training if maintained at home,patients health status remain above pre-rehabilitation levels.
- Oxygen Therapy– Long term O2 administration (>15 hours per day) to patients with chronic respiratory failure has been shown to increase survival in patients with severe,resting hypoxemia. Long term oxygen therapy is indicated for patients who have:
- PaO2 at or below 7.3 KPa or SaO2 at or below 88% with or without hypercapnia twice
over a 3week period. - PaO2 between 7.3 KPa & 8 KPa or SaO2 at or below 88%,if there is evidence of
pulmonary hypertension,peripheral edema or polycythemia.
- PaO2 at or below 7.3 KPa or SaO2 at or below 88% with or without hypercapnia twice
- Ventilatory Support-The combination of non-invasive ventilation with long term oxygen therapy may be of some use in selected patients,particularly in those with prolonged daytime hypercapnea.It may improve survival but does not improve quality of life.There are clear benefits of CPAP on both survival& risk of hospital admission.
- Surgical treatments– The advantage of lung volume reduction surgery over medical therapy is more significant among patients with upper lobe predominant emphysema & low exercise capacity prior to treatment,Although LVRS is costly relative to health care programs.In selective patients with very severe COPD patients lung transplantation has been shown to improve quality of life & functional capacity.
MANAGEMENT OF STABLE COPD
Once copd has been diagnosed,effective management should be based on an individualized assessment of current symptoms & future risks.the aims of treatment according to order of priority can be listed as follows
- Relieve symptoms
- Improve exercise tolerance
- Improve health status.
- Prevent disease progression
- Prevent & treat exacerbations
- Reduce mortality.
These goals should be reached with minimal side effects from treatment Because they commonly have comorbidities that also need to be carefully idenrtified & treated.
NON-PHARMOCOLOGICAL MANAGEMENT
| Patient Group | Essential | Recommended | Depending on local guidelines |
| A | Smoking Cessation(can include pharmac treatment) | Physical activity | Flu vaccination Pneumococcal vaccination |
| B, C, D | Smoking Cessation(can include pharmac treatment) Pulmonary Rehabilitation | Physical activity | Flu vaccination Pneumococcal vaccination |
PHARMACOLOGICAL THERAPY FOR STABLE COPD
| Patient Group | FIRST CHOICE | SECOND CHOICE | ALTERNATIVE CHOICE |
| A | Short acting anticholinergics OR Short acting beta2 agonist | Long acting anticholinergics OR Long acting beta2 agonist OR Short acting anticholinergics & Short acting beta2 agonist | Theophylline |
| B | Long acting anticholinergics OR Long acting beta2 agonist | Long acting anticholinergics AND Long acting beta2 agonist | Short acting anticholinergics AND /OR Short acting beta2 agonist |
| C | Long acting anticholinergics OR Inhaled steroids+Long acting beta2 agonist | Long acting anticholinergics AND Long acting beta2 agonist | PDE-4 Inhibitor Short acting anticholinergics AND /OR Short acting beta2 agonist Theophylline |
| D | Long acting anticholinergics OR Inhaled steroids+Long acting beta2 agonist | Inhaled steroids+ Long acting anticholinergics OR Inhaled steroids+Long acting beta2 agonist and Long acting anticholinergics OR Inhaled steroids+Long acting beta2 agonist and PDE-4 Inhibitor OR Long acting anticholinergics & Long acting beta2 agonist OR Long acting anticholinergics and PDE-4 Inhibitor | Carbocysteine Short acting anticholinergics AND /OR Short acting beta2 agonist Theophylline |
MANAGEMENT OF EXACERBATIONS
An Exacerbation of COPD is defined as an acute event characterized by worsening of patients respiratory symptoms that is beyond normal day to day variations & leads to change in medications.The most common cause appears to be respiratory tract infections(viral or bacterial).
Assessment of severity of an Exacerbation
- ABG measurement: PaO2 < 60 mm Hg with or without PaCo2 > 55mm Hg at breathing room air indicate respiratory failure.
- Chest X-ray are useful in excluding alternative diagnoses.
- An ECG may aid in diagnosing coexisting cardiac problems.
Spirometric tests are not recommended during an exacerbation because they can be difficult to perform & measurements may not be accurate.
Treatment Options
Oxygen– Supplemental oxygen should be titrated to improve patients hypoxemia with target SPO2 88-92%.
Bronchodilators-Short acting inhaled beta2 agonists with or without short acting anticholinergics are the preferred bronchodilators.
Systemic Steroids– systemic steroids shorten recovery time,improve lung function & arterial hypoxemia and reduce the risks of early relapse,treratment failure & length of hospital stay .A dose of 30-40 mg prednisolone per day for 10-14 days is recommended.
Antibiotics– should be given to patients
- With cardinal symptoms-Increased sputum volume, increased dyspnea, increased sputum purulence.
- With increased sputum purulence & one other cardinal symptom
- Who require mechanical ventilation
Adjunct therapies-Depending on clinical condition of the patient,an appropriate fluid balance with special attention to giving diuretics, anticoagulants, treatment of comorbidities,nutritional aspects should be considered.
COPD & SPECIFIC ISSUES
1. COPD and air travel
For most passengers, even those with respiratory disease, air travel is safe and comfortable. Some patients with COPD may be at risk but, with screening, these patients can be identified and most can travel safely with supplemental oxygen. Patients with respiratory disorders may be at risk for arterial hypoxia during air travel due to the decrease in ambient air pressure. Those with chronic obstructive pulmonary disease (COPD) are particularly vulnerable.
For patients with respiratory disorders whose oxygenation while breathing air may be marginal at sea level, the reduction of arterial PO2 and saturation at altitude may fall below the level of safety. The need for oxygen supplementation should be a consideration whenever the arterial oxygen saturation or pulse oxygenation falls to 84% or below.
2. COPD and surgery
Pulmonary complications in patients of COPD undergoing surgery are common, often serious when they occur and are costly to treat.The major pulmonary complications that clinicians seek to prevent through proper preoperative evaluation and intervention include pneumonia, prolonged mechanical ventilation or respiratory failure, atelectasis, bronchospasm, and exacerbations of chronic obstructive pulmonary disease.
Preop– Preoperative spirometry should be performed. Identification of severe airflow obstruction may be particularly important in patients who are candidates for upper abdominal or thoracic surgical procedures, in addition physical examination findings can be helpful in assessing risk magnitude, as Decreased breath sounds, prolonged expiration, rales, wheezes,and rhonchi alone may warrant increase in pulmonary complications compared with the absence of any of these findings.Since patients with COPD are at increased risk of pulmonary neoplasm and other pathologies, a preoperative chest radiography, if not recently performed, is reasonable. This recommendation is in keeping with the recommendations for the general assessment of COPD.
Analysis of arterial blood gas (ABG) composition should be available for patients with moderate-to-severe COPD. For patients who may require ventilatory assistance, knowledge of preoperative blood gases may be helpful in determining appropriate postoperative ventilator settings. Although ABG values need not be used as a sole determinant of general surgical candidacy, they may influence decision making for high-risk procedures.
What is equally important in preop period is ,very effort should be made to aid with smoking cessation. Smoking cessation at least 4-8 weeks preoperatively is optimal .Optimisation of lung function using inhaled bronchodilators in severe COPD can decrease postoperative complications,although oral corticosteroids are not recommended for chronic disease management in the patient with COPD, those who are taking these agents chronically should be treated with systemic steroids in the perioperative period to minimise the risk of adrenal insufficiency. Although the potential for adrenal insufficiency does exist in patients taking high-dose inhaled corticosteroids, the risk appears to be low in asthmatics. Pulmonary rehabilitation should be considered in high-risk patients undergoing elective procedures. Pre- and postoperative pulmonary rehabilitation have been shown to decrease postoperative pulmonary complications after abdominal surgery.
Remembe. COPD = increased risk (RR 2,7-4,7) of postoperative respiratory complications and Inhaled β2-agonists and inhaled anticholinergics should be continued up to the day of surgery.
Intraoperative
The COPD patient may be more sensitive to the ventilatory depressant effects of the analgesic, regional and general anaesthetic agents used .Volatile anesthetics, intravenous anaesthetics and neuromuscular blocking agents vary in their ability to provoke unwanted autonomic effects and alter airway reactivity. The risk of pulmonary complications may be higher with the use of the long-acting neuromuscular blocker pancuronium than shorter-acting atracurium or vecuronium.
The role of general versus regional anaesthesia remains controversial. A meta-analysis suggested that neuroaxial blockade with epidural or spinal anaesthesia decrease postoperative mortality, deep venous thrombosis, pulmonary embolism, transfusion requirements, pneumonia and respiratory depression . Thoracic epidural anaesthesia appears to have only limited deleterious effects on pulmonary function in patients with severe COPD and has been used as the primary mode of anaesthesia for COPD patients undergoing chest wall surgery, the combination of thoracic epidural and general anesthesia may result in less shunting and better oxygenation during thoracic surgical procedures.
Postoperative management of COPD: COPD doubles the risk of postoperative pulmonary complications and the severity of COPD influences postoperative pulmonary complication rates. Those with severe COPD are six times more likely to have major postoperative complication. .Close surveillance and Rapid detection of respiratory problems, need of Supplemental oxygen atracurium-mivacurium Respiratory failure, Inability to clear airway secretions, Lowered respiratory drive due to opioids should be watched for.
The immediate postoperative recovery period is a period of high risk because of the possibilities of respiratory muscle dysfunction, acidemia, hypoxaemia and hypoventilation. Close monitoring and, if necessary, mechanical ventilator support becomes crucial at this time . Suggested Ventilator strategy to reduce dynamic hyperinflation: Allow more time to exhale,- Decrease respiratory rate,- Decrease I:E ratio,- Allow permissive hypercapnia,- Increase inspiratory flow rate and tolerate higher peak pressures,Apply Extrinsic PEEP.
In patients with COPD and reduced airflow, complication rates vary with the region of the body upon which surgery is performed. The further the procedure from the diaphragm, the lower the risk .Early mobilisation, deep breathing, intermittent positive-pressure breathing or incentive spirometry have been reported to decrease postoperative complications after upper abdominal surgery .A necessary component of postoperative management is effective analgesia. Epidural administration may offer superior analgesia with less sedation by promoting patient mobility and deep breathing.Indications for postoperative mechanical ventilation are respiratory failure with retained secretions, atelectasis and pneumonia .Continuation of preoperatively prescribed respiratory medications is standard therapy.
Weaning from mechanical ventilation patients with COPD who have had cardiac surgery may be prolonged . The patient should be ventilated at a level that maintains arterial carbon dioxide tension at the preoperative level with a normal pH. In the COPD patient who is difficult to extubate, gradual weaning may permit the patient’s cardiovascular status to become sufficiently stable to tolerate assumption of the full work of breathing. In this group of patients, early consultation with an intensivist or pulmonologist may optimise weaning.
References:
- 1.Agusti AG. Systemic effects of chronic obstructive pulmonary disease. Proc Am Thorac Soc2005;2(4):367-70.
- Johannessen A, Lehmann S, Omenaas ER, Eide GE, Bakke PS, Gulsvik A. Post-bronchodilator spirometry reference values in adults and implications for disease management. Am J Respir Crit Care Med 2006;173(12):1316-25.
- Stoller JK, Aboussouan LS. Alpha1-antitrypsin deficiency.Lancet 2005;365(9478):2225-36.
- Sundeep salvi, editorial, JAPI vol. 601. Salvi S. COPD: The neglected epidemic. Textbook of Pulmonary and Critical Care Med Vol 2, Ed: Jindal SK, Jaypee Publications, 2011;971-974.
- The Global burden of Disease, WHO 2008 Oct, http://www.who.int/healthinfo/global_burden_disease/projections/en/index.html. accessed on 22nd Dec 2011.
- Lopez A, Shibuya K, Rao C et.al. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J2006;27:397-412
- 7. Health Status Maharashtra 2009: A report by the State Health Systems resource Centre. 2010;20-21
- US Surgeon General. The health consequences of smoking:chronic obstructive pulmonary disease. Washington, D.C.: US Department of Health and Human Services; 1984.
- Burrows B, Knudson RJ, Cline MG, Lebowitz MD. Quantitative relationships between cigarette smoking and ventilatory function.Am Rev Respir Dis 1977;115(2):195-205.
- Becklake MR. Occupational exposures: evidence for a causal association with chronic obstructive pulmonary disease. Am Rev Respir Dis 1989;140(3 Pt 2):S85-91.
- Trupin L, Earnest G, San Pedro M, Balmes JR, Eisner MD,Yelin E, et al. The occupational burden of chronic obstructive pulmonary disease. Eur Respir J 2003;22(3):462-9.
- Matheson MC, Benke G, Raven J, Sim MR, Kromhout H,Vermeulen R, et al. Biological dust exposure in the workplaceis a risk factor for chronic obstructive pulmonary disease.Thorax 2005;60(8):645-51.
- Hnizdo E, Sullivan PA, Bang KM, Wagner G. Association between chronic obstructive pulmonary disease and employmentby industry and occupation in the US population: a study of data from the Third National Health and Nutrition Examination Survey. Am J Epidemiol 2002;156(8):738-46.
- Warwick H, Doig A. Smoke the killer in the kitchen: Indoor air pollution in developing countries. ITDG Publishing, 103-105 Southampton Row, London WC1B HLD, UK 2004:URL: http://www.itdgpublishing.org.uk.
- Ezzati M. Indoor air pollution and health in developing countries. Lancet 2005;366(9480):104-6.
- Smith KR, Mehta S, Maeusezahl-Feuz M. Indoor air-pollution from household solid fuel use. In: Ezzati, M., Lopez, A. D.,Rodgers, M., Murray, C. J., eds. Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors. Geneva: World Health Organization; 2004.
- Mishra V, Dai X, Smith KR, Mika L. Maternal exposure to biomass smoke and reduced birth weight in Zimbabwe. Ann Epidemiol 2004;14(10):740-7.
- Boman C, Forsberg B, Sandstrom T. Shedding new light on wood smoke: a risk factor for respiratory health. Eur Respir J2006;27(3):446-7.
- Oroczo-Levi M, Garcia -Aymerich J, Villar J, Ramirez-Sarmiento A, Anto JM, Gea J. Wood smoke exposure and risk of chronic obstructive pulmonary disease. Eur Respir J 2006;27:542-6.
- Sezer H, Akkurt I, Guler N, Marakoglu K, Berk S. A case-control study on the effect of exposure to different substances on the development of COPD. Ann Epidemiol 2006;16(1):59-62.
- Barker DJ, Godfrey KM, Fall C, Osmond C, Winter PD,Shaheen SO. Relation of birth weight and childhood respiratory infection to adult lung function and death from chronic obstructive airways disease. BMJ 1991;303(6804):671-5.
- Todisco T, de Benedictis FM, Iannacci L, Baglioni S, Eslami A, Todisco E, et al. Mild prematurity and respiratory functions.Eur J Pediatr 1993;152(1):55-8.
- Stein CE, Kumaran K, Fall CH, Shaheen SO, Osmond C,Barker DJ. Relation of fetal growth to adult lung function in South India. Thorax 1997;52(10):895-9.
- Barnes PJ, Shapiro SD, Pauwels RA. Chronic obstructive pulmonary disease: molecular and cellular mechanisms. Eur Respir J 2003;22(4):672-88.
- Hogg JC. Pathophysiology of airflow limitation in chronic obstructive pulmonary disease. Lancet 2004;364(9435):709-21
- Rahman I. Oxidative stress in pathogenesis of chronic obstructive pulmonary disease: cellular and molecular mechanisms.Cell Biochem Biophys 2005;43(1):167-88.
- MacNee W. Oxidative stress and lung inflammation in airways disease. Eur J Pharmacol 2001;429(1-3):195-207.
- Barnes PJ. Mediators of chronic obstructive pulmonary disease. Pharmacol Rev 2004;56(4):515-48.
- Thomson NC, Chaudhuri R, Livingston E. Asthma and cigarette smoking. Eur Respir J 2004;24(5):822-33
- Hogg JC, Chu F, Utokaparch S, Woods R, Elliott WM, BuzatuL, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med 2004;350(26):2645-53.
- O’Donnell DE, Revill SM, Webb KA. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2001;164(5):770-7.





