Haematologist & Medical Oncologist & BMT Consultant,
Director, Central India Institute of Haematology & Oncology (CIIHO)
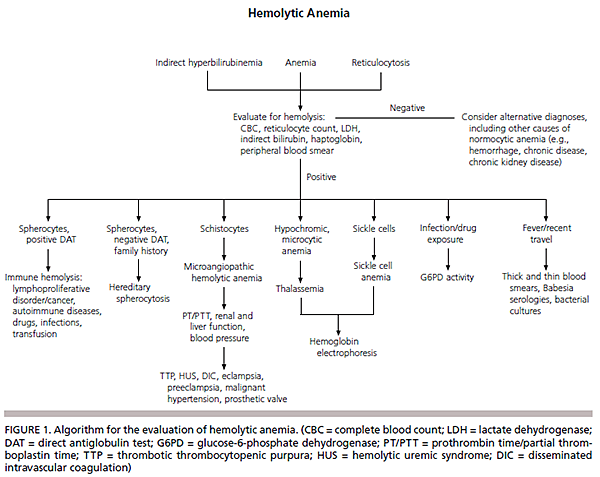
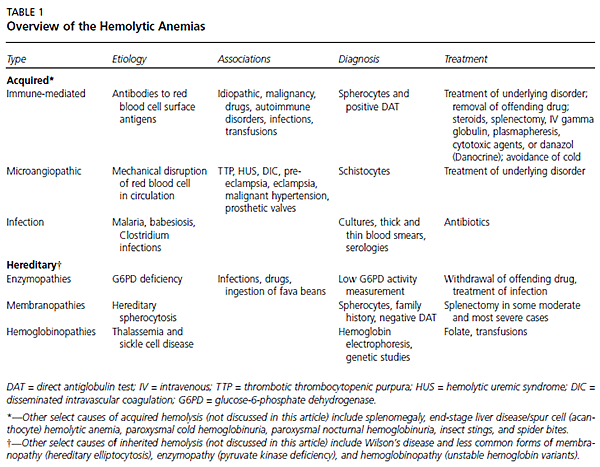
Hemolysis is the destruction or removal of red blood cells from the circulation before their normal life span of 120 days. While hemolysis can be a lifelong asymptomatic condition, it most often presents as anemia when erythrocytosis cannot match the pace of red cell destruction. Hemolysis also can manifest as jaundice, cholelithiasis, or isolated reticulocytosis.
Pathophysiology
There are two mechanisms of hemolysis. Intravascular hemolysis is the destruction of red blood cells in the circulation with the release of cell contents into the plasma. Mechanical trauma from a damaged endothelium, complement fixation and activation on the cell surface, and infectious agents may cause direct membrane degradation and cell destruction. The more common extravascular hemolysis is the removal and destruction of red blood cells with membrane alterations by the macrophages of the spleen and liver. Circulating blood is filtered continuously through thin walled splenic cords into the splenic sinusoids (with fenestrated basement membranes), a spongelike labyrinth of macrophages with long dendritic processes.1 A normal 8-micron red blood cell can deform itself and pass through the 3-micron openings in the splenic cords. Red blood cells with structural alterations of the membrane surface (including antibodies) are unable to traverse this network and are phagocytosed and destroyed by macrophages.
History and Physical Examination
Anemia most often is discovered through laboratory tests, but the history and physical examination can provide important clues about the presence of hemolysis and its underlying cause. The patient may complain of dyspnea or fatigue (caused by anemia). Dark urine and, occasionally, back pain may be reported by patients with intravascular hemolysis. The skin may appear jaundiced or pale. A resting tachycardia with a flow murmur may be present if the anemia is pronounced. Lymphadenopathy or hepatosplenomegaly suggest an underlying lymphoproliferative disorder or malignancy; alternatively, an enlarged spleen may reflect hypersplenism causing hemolysis. Leg ulcers occur in some chronic hemolytic states, such as sickle cell anemia.
Diagnostic Testing
HEMATOLOGIC TESTS
Along with anemia, a characteristic laboratory feature of hemolysis is reticulocytosis, the normal response of the bone marrow to the peripheral loss of red blood cells. In the absence of concomitant bone marrow disease, a brisk reticulocytosis should be observed within three to five days after a decline in hemoglobin. In a minority of patients, the bone marrow is able to chronically compensate, leading to a normal and stable hemoglobin concentration. The anemia of hemolysis usually is normocytic, although a marked reticulocytosis can lead to an elevated measurement of mean corpuscular volume, because the average mean corpuscular volume of a reticulocyte is 150 fL.2 Review of the peripheral blood smear is a critical step in the evaluation of any anemia. Along with an assessment for pathognomonic red blood cell morphologies, such as spherocytes or schistocytes, examination of the white blood cells and platelets for coexisting hematologic or malignant disorders is essential.
CHEMISTRY TESTS
The destruction of red blood cells is characterized by increased unconjugated bilirubin, increased lactate dehydrogenase, and decreased haptoglobin levels. Lactate dehydrogenase and hemoglobin are released into the circulation when red blood cells are destroyed. Liberated hemoglobin is converted into unconjugated bilirubin in the spleen or may be bound in the plasma by haptoglobin. The hemoglobin-haptoglobin complex is cleared quickly by the liver, leading to low or undetectable haptoglobin levels.
URINARY TESTS
In cases of severe intravascular hemolysis, the binding capacity of haptoglobin is exceeded rapidly, and free hemoglobin is filtered by the glomeruli. The renal tubule cells may absorb the hemoglobin and store the iron as hemosiderin; hemosiderinuria is detected by Prussian blue staining of sloughed tubular cells in the urinary sediment approximately one week after the onset of hemolysis. Hemoglobinuria, which causes red-brown urine, is indicated by a positive urine dipstick reaction for heme in the absence of red blood cells.