
Associate Professor, Anesthesiology,
Govt. Medical College & Superspeciality Nagpur
Anesthetizing patients with “reactive airway” remains a challenge to the anesthesiologist. There is always a possibility of catastrophic bronchospasm and other respiratory complications associated with anesthesia in patients with reactive airways. Anesthesiologist has to be selective regarding the choice of anesthesia technique and the use of drugs in these patients to avoid the provocation of bronchospasm and other airway related complications and if it occurs should recognize and manage appropriately.
“Reactive airways” and “reactive airways disease” are highly nonspecific terms. Patients are usually labeled with “reactive airways” if they have a history of cough, sputum production, wheeze, or dyspnea. The term “reactive airway disease” has been used differently. In one instance reactive airway disease was used as a summary term to describe patients with asthma and/or COPD; in the other it was used synonymously with airway hyperreactivity (1,2)
Airway hyperreactivity is a specific term that means that the airways are hyperreactive to a variety of stimuli including methacholine, histamine, hypertonic saline, distilled water, exercise, or eucapnic hyperventilation. Hyperreactivity in this context means a bronchoconstrictor response at “doses” that normally have no bronchoconstrictor effect. Airway hyerreactivity actually encompasses both airway sensitivity (the dose of agonist at which the FEV1 begins to fall) and airway hyperresponsiveness (the slope of the dose–response curve thereafter).(3) The mention of such airway hyperactivity immediately focuses on the asthmatic with intermittent bouts of severe airflow obstruction. However, it is important to emphasize that heightened airway reactivity also occurs in patients with chronic bronchitis and emphysema as well as allergic rhinitis and upper and lower respiratory tract infections. The latter patients may actually be more at risk for perioperative bronchospasm than many asthmatics.(4) Indeed, Warner et al. found a surprisingly low frequency of perioperative bronchospasm in patients with asthma. (5).
Mechanisms Of Airway Hyperactivity (4)
A mild tonic constriction exists in all normal human airways. This is largely maintained by efferent vagal activity and is readily abolished by antimuscarinics such as atropine. The physiological importance of this normal resting tone is an airway size that provides balance between anatomic dead space and airway resistance to gain efficiency in both gas exchange and work of breathing (Fig. 1).
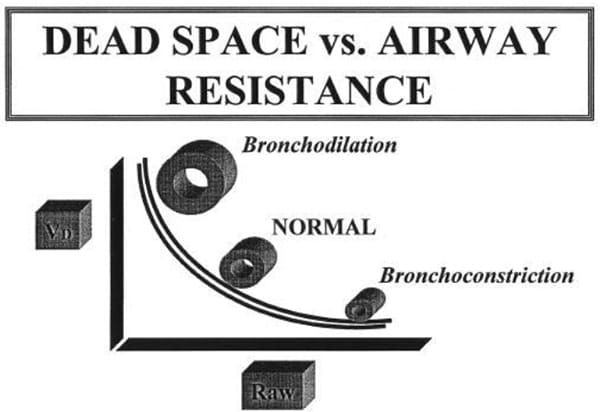
Figure 1. Relationship between anatomic airway dead space (Vd) and airway resistance (Raw) in the normal control state and after bronchodilation and bronchoconstriction. Note that with bronchodilation as Raw decreases Vd increases, whereas with bronchoconstriction Vd decreases as Raw increases.
(From – http://www.iars.org/2002ReviewCourseLectures/pdfs/gal2002.pdf)
The exaggerated responses of patients with airway disease have been ascribed to numerous factors like reduced resting airway caliber, presence of mucosal edema and inflammation and the volume of airway secretions. Airway hyperactivity has often been depicted as a simple autonomic imbalance with a relatively increased parasympathetic activity in the lung. Sympathetic innervation in the lung is very limited and difficult to identify. Instead, the major sympathetic influence on airway caliber occurs via circulating catecholamines that act primarily on the β2-receptors to produce bronchodilation. The parasympathetic nervous system controls both the baseline tone as well as the rapid changes in airway caliber in response to airway stimulation. Within the airway wall sensory receptors alter bronchial smooth muscle tone through the parasympathetic vagal pathways. The most important of these are the rapidly adapting irritant receptors found throughout the mucosa of all the cartilaginous airways but most prominent in the trachea and especially at the carina. They respond to mechanical irritation, thermal stimuli, and irritants such as inhaled particle of gases. Airway edema and histamine reflexes also elicit their activity, which results in reflex cough, bronchoconstriction, and mucus secretion.
Identifying Patients with Reactive Airways
Preoperative identification of patients with reactive airways is important in planning a rational approach for anesthetic care. Respiratory symptoms, highly predictive of increased bronchial reactivity, consist principally of nocturnal dyspnoea and chest tightness on awakening and an associated breathlessness and wheezing in response to various respiratory irritants such as cold air. History of a upper and lower respiratory infection, cough, sputum production, wheeze, increases the likelihood of perioperative bronchospasm. It is well recognized that the clinical state of asthmatic and bronchitic patients often deteriorates markedly when they suffer viral respiratory tract infections.
In normal subjects, viral upper respiratory infections cause a striking increase in bronchial reactivity that appears to persist for 3 to 4 wks. after infection (6).
Examination may be normal in a well-controlled asthmatic patient, but may reveal chest hyperinflation, prolonged expiratory phase and wheeze.
Preoperative management in asthmatics should include the following measures. (7)
- Bronchospasm should be treated with inhaled β2-agonists;
- If a patient is at risk for complications, preoperative treatment with 40-60 mg of prednisone/day or hydrocortisone 100 mg every 8 h intravenously is suggested. Anyone with a preoperative FEV1<80% of predicted should receive steroids;
- Infections should be eradicated using antibiotics;
- Fluid and electrolyte imbalances should be corrected, given that high dose β2-agonists can cause hypokalemia, hyperglycemia, and hypomagnesemia. In addition to that imbalance, there may be a decreased response to β2-agonists and predisposition to cardiac arrhythmias;
- Prophylactic cromolyn treatment to prevent degranulation of mast cells and release of mediators should be continued;
- Chest physiotherapy improves sputum clearance and bronchial drainage;
- Other conditions such as cor pulmona pulmonale should be treated;
- The patient should stop smoking in order to reduce carboxyhemoglobin levels.
Cessation of smoking is followed by a decreased volume of airway secretions, less airway reactivity, and improved mucociliary transport, but these benefits take several weeks to develop (8). In the short term (48–72 h) there may actually be increased reactivity and secretions such that the only actual benefit may be the decrease in carboxyhemoglobin content and thus better oxygen delivery to the tissue (9).
Clearly document any allergies or drug sensitivities, especially the effect of aspirin or other non-steroidal anti-inflammatory drug (NSAIDs) on asthma.
In asthmatics serial measurements of peak flow are more informative than a single reading. ‘Early morning dip’ in peak flow readings or > 20% variability in Peak Expiratory Flow Rate (PEFR), suggests control is not optimal. Spirometry gives a more accurate assessment. Measure response to bronchodilators. Blood gases are only necessary in assessing patients with severe asthma (poorly controlled, frequent hospital admissions, previous ICU admission), particularly prior to major surgery
Pharmacologic Therapy (4):
Parasympathetic innervation provides the major influence on airway smooth muscle by releasing acetylcholine onto muscarinic receptors and causing contraction and an increase in airway secretions. Sympathetic innervation of airway is sparse and difficult to identify. . Instead, the major sympathetic
influence on airway caliber occurs via circulating catecholamines that act primarily on the B2-receptors to produce bronchodilation. Nevertheless, the major therapeutic efforts for dealing with bronchial reactivity have employed drugs with sympathetic activity.
β-Adrenergics
These drugs form the cornerstone of therapy for prophylaxis as well as reversal of bronchospasm. At present, albuterol (salbutamol) is still the most popular because of its marked β2 selectivity, i.e., bronchial smooth muscle relaxation occurs with little or no undesirable β1 effects such as tachyarrhythmia. Much of the β2 selectivity results from the aerosol route of administration and the local deposition in the airways to produce bronchodilation. If given IV, albuterol is less effective as a bronchodilator, and the plasma concentrations needed effectively abolish β2 selectivity (10)
β -blockers in the presence of reactive airway disease –The treatment of tachycardia, hypertension, or angina pectoris with such drugs can precipitate or worsen bronchoconstriction. The replacement of propranolol with more cardio selective β –blockers atenolol or metoprolol can reduce, but not eliminate, the risk.
Methylxanthines
Theophylline and its relatives, are the mainstays of chronic bronchodilator therapy. Aminophylline, the ethylene-diamine watersoluble salt of the theophylline, is roughly 80% theophylline. Despite its rather narrow therapeutic range, aminophylline is considered the standard maintenance therapy in patients with airflow obstruction. Its role in treating acute bronchospasm has been increasingly questioned. Meta-analysis has underscored the scarcity of data supporting the rational use and efficacy of aminophylline for treatment of acute bronchospasm in the emergency setting (11)
Corticosteroids
Parenteral steroids are used as adjuncts in preoperative preparation of patients with reactive airway disease and during treatment of intraoperative bronchospasm. Dosage equivalents of 1–2 mg/kg hydrocortisone are usually recommended. Steroids suppress airway inflammation, mucous secretion, and the release of activity of mediator substances. They also appear to enhance and prolong the therapeutic effects of the β-adrenergic agonists. Preoperative administration is particularly important because the airway effects require some time to develop.
Concerns about negative effects of perioperative treatment with corticosteroids in terms of wound healing and infection were not supported by studies in asthmatic patients receiving prophylactic treatment with corticosteroids perioperatively, and there is evidence that asthmatic patients who are treated with corticosteroids can undergo surgical procedures with a low incidence of complications.(12)
Other Anti-Inflammatory Agents
Cromolyn and nedocromil, that inhibit mast cell release of histamine and other substances are important, particularly in asthmatics. These drugs, however, have no actual bronchodilating effect. They merely inhibit bronchoconstriction.
Anticholinergic Agents
They offer an alternative or complementary therapy for airway obstruction, especially in patients who experience tremor or tachycardia with β-adrenergic drugs. Ipratropium bromide is available as metered dose aerosol.
Glycopyrrolate, familiar to anesthesiologists, produces prolonged bronchodilation when injected IV or inhaled as an aerosol (13). Large doses of glycopyrrolate are required to prevent or reverse reflex bronchospasm although maximal bronchodilation occurs with considerably lower doses in normal patients (14). The maximum bronchodilating action of the anticholinergics is somewhat slow in onset (20–30 min) whether by inhalation or parenteral administration. Thus, they are more useful as prophylaxis than as treatment for active episodes of bronchospasm (15). Such prophylaxis can be readily accomplished by IV administration, ideally 20 to 30 min before induction of anesthesia.
Effects of Anesthetic agents on airway
Inhalation anesthetics such as halothane produce bronchodilation and appear to prevent the development of bronchospasm. The major effect on airway caliber is the result of blocking airway reflexes and direct relaxing effects on airway smooth muscle (16).
Halothane has long been considered the agent of choice but its myocardial depressant action and arrhythmic effects in the presence of circulating catecholamines are limitations. Both enflurane and isoflurane equally prevented vagally medicated bronchoconstriction at equal multiples of MAC (17). Because such anesthetic levels (>1.5 MAC) may be difficult to achieve in some patients because of cardiovascular depression, other adjunct therapy for bronchospasm must be considered. Laboratory evidence suggests that at lower doses of anesthetic (<1.0 MAC), halothane may be the most effective agent in reversing airway constriction. On the other hand, clinical observations in humans indicate that sevoflurane at 1.1 MAC may be the most effective agent, especially in the presence of airway instrumentation (18). Desflurane, on the other hand, has little utility and may elicit bronchoconstriction in smokers (19).
IV Induction Agents
Customary hypnotic doses of thiopental leave airway reflexes largely intact, and bronchospasm may occur if instrumentation of the airway is attempted. It has long been recognized that thiopental per se was not the cause of bronchospasm and is therefore not contraindicated in patients with airway disease. However propofol, another short-acting anesthetic, may be useful for induction of anesthesia in the patient at risk for bronchospasm largely because of profound depression of airway reflexes. Pizov et al. observed that both asthmatic and nonasthmatic patients who received a thiobarbiturate for induction had a greater incidence of wheezing than did patients receiving propofol.(20) Ketamine an i.v. general anaesthetic is considered an attractive choice, where appropriate, because of its sympathomimetic bronchodilatory properties and its effectiveness at preventing and reversing wheezing in patients with asthma who require anaesthesia and intubation. Ketamine may increase airway secretions. Etomidate, however, is as ineffective as thiopental in blunting airway reflexes (21).
Local Anesthetics
IV lidocaine have occasionally been suggested as part of the treatment of airway reactivity and intraoperative bronchospasm. Major mechanism whereby lidocaine prevent bronchospasm was by blockade of the airway reflex response to irritation and a direct smooth muscle action. Aerosol therapy offers little or no advantage over IV administration and may itself provoke bronchospasm because of direct airway irritation. Pretreatment with IV lidocaine may blunt constriction response and enhance subsequent bronchodilation as well (22)
Muscle Relaxants
Muscle relaxants can affect airway calibre and reactivity by promoting histamine release( atracurium, mivacurium, d-tubocurarine ) or by interacting with muscarinic receptors as structural analogs of acetylcholine. Perhaps, a more important factor with regard to the use of muscle relaxants concerns the need to reverse their actions. By inhibiting the destruction of endogenous ACH, cholinesterase inhibitors such as neostigmine may increase airway secretions and can precipitate bronchospasm. These effects can be prevented by muscarinic antagonists, and it seems prudent to use larger than the customary doses of glycopyrrolate (0.5 mg) or atropine (1.0 mg) to minimize the possible muscarinic side effects of reversal. An alternate approach would be to avoid the need for reversal by infusing short acting relaxants.
Anesthetic management
Anesthesia can precipitate life threatening bronchospasm in patients with reactive airways disease (e.g. asthmatics and COPD patients). This can be due to anxiety, anesthetic drugs, and airway manipulation. Anesthetics also worsen mucus trapping by drying secretions and impairing cilial function. Any patient who has been on steroids in the previous 6 months will need steroid replacement to cover the stress of surgery since there may still be a degree of adrenal suppression.
Whenever feasible, regional anesthesia constitutes an ideal choice in the patient with reactive airway disease because it eliminates the need for airway instrumentation and the possibility of eliciting airway reflexes. However, if high levels of sensory and motor block are required they may produce severe anxiety and actually incite bronchospasm. Also, the loss of expiratory muscle power may functionally limit some patients with airway obstruction not only in their ability to cough but also because of their need for active exhalation. Another concern with the high sensory and motor blockade with regional anesthesia is the associated blockade of sympathetic input to the lungs (4). Some case reports have speculated about a resultant increase in airway resistance. Groeben et al. (23) dispelled this notion and actually provided evidence that systemic levels of the local anesthetic associated with epidural anesthesia actually attenuated airway hyperreactivity.
Prevention Of Bronchospasm
Patients with asthma and COPD should have their airways disease under optimal control prior to elective surgery and should continue their inhalers and steroids up until the day of surgery. Wheezing, cough, increased sputum production, shortness of breath and diurnal variability in peak expiratory flow rate (PEFR) indicate poor control. Recent or frequent exacerbations or admission to hospital and history of a recent upper respiratory infection may be an indication to postpone non-essential surgery. All patients should and encouraged to stop smoking preoperatively. Six to eight weeks of abstinence before surgery significantly reduces the risk of respiratory complications including bronchospasm. Pretreatment with an inhaled/nebulised beta agonist, 30 minutes prior to surgery, induction of anaesthesia with propofol and adequate depth of anaesthesia before airway instrumentation reduces the risk of bronchospasm Tracheal intubation should not be attempted early unless adequate depth of anaesthesia is achieved. Because clinical studies suggest much of the bronchoconstriction occurs thorough vagal reflexes, pretreatment with vagal blocking doses of atropine or glycopyrrolate before induction of general anesthesia may be valuable. IV lidocaine (1–2 mg/kg) can also be used as therapeutic adjuncts to prevent reflex airway constriction. . The use of an LMA (in suitable patients) has been shown to reduce the incidence of bronchospasm compared to tracheal intubation.
Certain surgical procedures have highly stimulating stages that can trigger bronchospasm (and laryngospasm). Examples of these include anal or cervical dilatation, stripping of the long saphenous vein during varicose vein surgery and traction on the peritoneum. These are often predictable and can be prevented or countered by an intravenous bolus of opioid and/or anaesthetic agent such as propofol. Certain volatile anaesthetic agents (isoflurane, desflurane) if introduced quickly can trigger bronchospasm. IV agents including beta-blockers, prostaglandin inhibitors (NSAIDs) and cholinesterase inhibitors (neostigmine), histamine release (thiopentone, atracurium, mivacurium, morphine, d-tubocurarine) can also precipitate bronchospasm; care should be taken with these drugs in higher risk patients.
Intraoperative Bronchospasm
In patients with well-controlled asthma and COPD the incidence is approximately 2%. The overall incidence of bronchospasm during general anaesthesia is approximately 0.2% (24)
Diagnosis (25)
Bronchospasm during anaesthesia usually manifests as prolonged expiration/ expiratory wheeze. Wheezing requires movement of gas through narrowed airways and so in severe bronchospasm wheeze is absent. Similarly, breath sounds may be reduced or absent. With IPPV, peak airway pressures are increased, tidal volumes reduced, or both. With capnography, narrowed airways and prolonged expiration result in a delayed rise in end-tidal carbon dioxide, producing a characteristic ‘sharkfin’ appearance (Figure 2)
Figure 2. The characteristic ‘shark-fin’ capnograph suggestive of airway obstruction
Positive pressure ventilation delivered before exhalation is complete can result in ‘breath-stacking’ and the development of an intrinsic (or auto) positive end-expiratory pressure (iPEEP or autoPEEP). Intrinsic PEEP can increase intrathoracic pressure, decrease venous return and impair cardiac output. Bronchospasm is not the only cause of wheeze or increased peak airway pressures during anaesthesia which should be looked for and ruled out.
Management Of Intraoperative Bronchospasm (25)
- Switch to 100% oxygen
- Ventilate by hand
- Stop stimulation / surgery
- Consider allergy / anaphylaxis; stop administration of suspected drugs / colloid / blood products
Increasing the inspired concentration of all volatile anaesthetic agents will produce bronchodilatation (the exception is esflurane, which at higher alveolar concentrations has been shown to increase airway resistance). If bronchospasm is severe, the effective delivery of volatile anaesthetic agents will be difficult. An intravenous agent may be necessary and propofol is desirable as it obtunds airway reflexes. ketamine also produces bronchodilatation.
In the first instance treatment is with an inhaled beta agonist such as salbutamol which produce more rapid and effective bronchodilatation than IV aminophylline, an often incorrectly listed therapy. This can be repeated . Administration must be downstream of the heat and moisture exchange filter (HMEF) and can be with an in-line adaptor, (Figure 3), nebuliser, or if these are not available, the metered dose inhaler (MDI) can be placed in the barrel of a 60ml syringe, the plunger replaced and a 15cm length of IV tubing attached to the end by Luer lock (Figure 4). This tubing is then fed down the ETT and reduces the deposition of aerosol on the tracheal tube. As an emergency, the MDI can be discharged directly down the ETT although much of the aerosol will not reach the patient’s airways
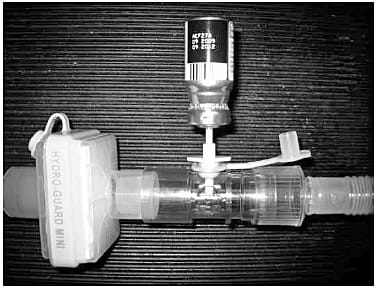
Figure 3. A metered dose inhaler (MDI) adaptor fitted in the breathing circuit, on the patient side of the heat and moisture exchanger. Depress the canister by hand during inspiration to administer the drug
(From-Update in Anaesthesia | www.anaesthesiologists.org –Management of bronchospasm during general anaesthesia)

Figure 4. An MDI canister can be placed in the barrel of a 60ml syringe and a 15cm length of IV tubing attached via the Luer lock. Feed the tubing down the ETT and press the plunger to administer the drug, then reconnect the breathing circuit and ventilate
(From-Update in Anaesthesia | www.anaesthesiologists.org –Management of bronchospasm during general
anaesthesia)
If the indication for surgery is not life-threatening, consider abandoning surgery, especially if
there is ongoing difficulty with ventilation, falling oxygen saturations or haemodynamic
compromise. In a non-intubated patient with severe bronchospasm, it may be necessary to
intubate the trachea and mechanically ventilate the lungs while therapy is initiated. If this is
the case then avoidance of histamine release is important and an appropriate muscle relaxant
should be used (e.g. rocuronium or vecuronium ).. In anesthetized patients skeletal muscle relaxation is essential because vigorous expiratory efforts may further increase airway pressures. Paralysis also helps to determine whether the increased airway pressure and difficulty in ventilating are caused by actual bronchospasm or merely straining and coughing on the endotracheal tube. Therapy with IV glycopyrrolate up to 1 mg may be helpful in reversing some of the reflex bronchoconstriction but is more valuable as prophylaxis because of its delay in onset. Direct instillation of glycopyrrolate through the endotracheal tube incurs a similar delay but has the advantage of avoiding systemic side effects. IV lidocaine (1.5–2 mg/kg) is also likely to be more effective if given before the stimulus, as would corticosteroids (hydrocortisone 4 mg/kg or its equivalent). Episodes of bronchospasm may be accompanied by arterial hypotension, often as a consequence of the high airway pressures necessary to achieve ventilation. In such cases IV ephedrine, an old reliable vasopressor is very useful because of its bronchodilating qualities. Similarly, IV epinephrine in doses of 10–20 mcg may be appropriate, especially if delivery of β-adrenergic aerosols is difficult. A common example of the latter is with a double-lumen tube in place.(4)
Drug doses for use in bronchospasm (25)
| Drug | Adult dose | Paediatric dose |
| Salbutamol | MDI (metered dose inhaler) 6-8 puffs Nebulised – 1ml 0.5% (5mg) IV – 250mcg slow IV then 5mcg.min -1 | MDI 6-8 puffs |
| Epinephrine titrated to response | IV-10mcg-100 mcg (0.1-1.0 ml 1:10,000) IM – 0.5-1.0mg if no IV access Nebulised 5ml 1:1000 | IV – 0.1-1.0 mcg.kg-1 (0.01- 0.1ml.kg-1 of 1:100,000) IM – <6 months 50mcg, 6 mths-6yrs 120mcg , 6-12 yr 250mcg, >12yrs 500mcg Nebulised 0.5ml.kg-1 1:1000 (max 5mls) |
| Ipratropium bromide | Nebulised 0.5mg 6 hourly | Nebulised (2-12yrs) 0.25mg 6 hourly |
| Magnesium sulphate | 2g IV over 20min (unlicenced) | 50mg.kg-1 IV over 20min (max 2g, unlicensed) |
| Ketamine Infusion | 1-3mg.kg-1.h-1 Bolus dose: 10-20mg | Infusion: 1-3mg.kg-1.h-1 |
| Aminophylline | 5mg.kg-1 IV over 20min then 0.5mg.kg-1.h -1 Infusion Omit loading dose if taking theophylline | 5mg.kg-1 IV over 20min then 1mg.kg-1.h-1 (<9yrs), 0.8mg.kg-1.h-1 (9-16yrs) infusion Omit loading dose if taking theophylline |
| Hydrocortisone | 200mg IV 6 hourly | <1yr 25mg, 1-5yrs 50mg, 6-12yrs 100mg 6 hourly |
Pregnant asthmatic and parturients undergoing anesthesia are at increased risk, especially if regional anesthetic techniques are not suitable and prostaglandin and its derivates are administered for abortion or operative delivery
Mechanical ventilation
The primary aim of mechanical ventilation in acute bronchospasm is to prevent or correct hypoxaemia. Tidal volumes may need to be reduced to avoid high peak airway pressures and barotrauma. Hypercapnia is tolerated if oxygenation is adequate, as long as severe acidosis does not develop (pH<7.15). Ventilation should incorporate a long expiratory time to allow complete exhalation and reduce ‘breath-stacking’ and intrinsic PEEP. Minimising intrinsic PEEP is best achieved with a slow respiratory rate, an inspiratory:expiratory ratio of at least 1:2. If bronchospasm is severe, only 3-4 breaths per minute may be possible if you allow full expiration
Child with URI for Anesthesia
One of the most controversial issues in pediatric anesthesia is whether to proceed with anesthesia and surgery in a child with an upper respiratory tract infection (URI). URI and URI-like symptoms of noninfectious etiology, such as allergic or vasomotor rhinitis in a child make the airway hyperreactive. Airway reactivity persists for 4 – 6 weeks following URI.
Many studies agree that children with active URI or recent URI are at increased risk for perioperative complications like laryngospasm, bronchospasm, breath holding, airway obstruction, apnea, major arterial desaturation (SpO2< 90% ), severe coughing, post-extubation stridor and atelectasis. Although most studies agree that children with active and recent URIs are at increased risk for perioperative complications, these events, for the most part, are manageable and have no long-term adverse sequelae. Some children, have such frequent URIs that to find a disease free window is impossible. Considering the emotional and financial burden on parents and, after identifying the factors that place the child with URI at risk, anesthesiologists are now in a better position to make informed decisions regarding the suitability of proceeding with surgery for these children. Hence blanket cancellation of surgery of a child with URI has now become a thing of the past.
With the availability of better anesthetic drugs, frequent use of regional anesthesia in children, can further reduce incidence of airway related complications in children with uncomplicated URIs.
Tait et al. (26) examined the incidence of and risk factors for adverse respiratory events in 1078 children undergoing a variety of surgical procedures. Results showed that children with active and recent URIs (in the last 4 wk) had significantly more episodes of overall respiratory events, breath-holding, major arterial oxygen desaturation (SpO2 <90%), and severe coughing compared with children with no URIs. . Despite the increased risk of respiratory events in children with URIs, there appears to be very little residual morbidity. Indeed, there are no cases in the pediatric and adult anesthesia closed claims literature implicating URIs with serious adverse events (27).
Parnis et al. (28), in a study of 2051 pediatric surgical patients, identified 8 clinical predictors of anesthetic complications. These predictors included – airway management (endotracheal tube [ETT] > laryngeal mask airway [LMA] > face mask), the parents’ statement that the child had a “cold,” a history of snoring, passive smoking, induction anesthetic (thiopental > halothane > sevoflurane > propofol), presence of sputum, presence of nasal congestion, and use of an anticholinesterase (muscle relaxant not reversed > reversed).
Children less than 1 year of age ,prematurity, surgery involving airway, history of reactive airway disease has also been implicated as risk factors for airway complications in children with URI.
A suggested algorithm for the assessment and management of the child with a URI is presented.(27)
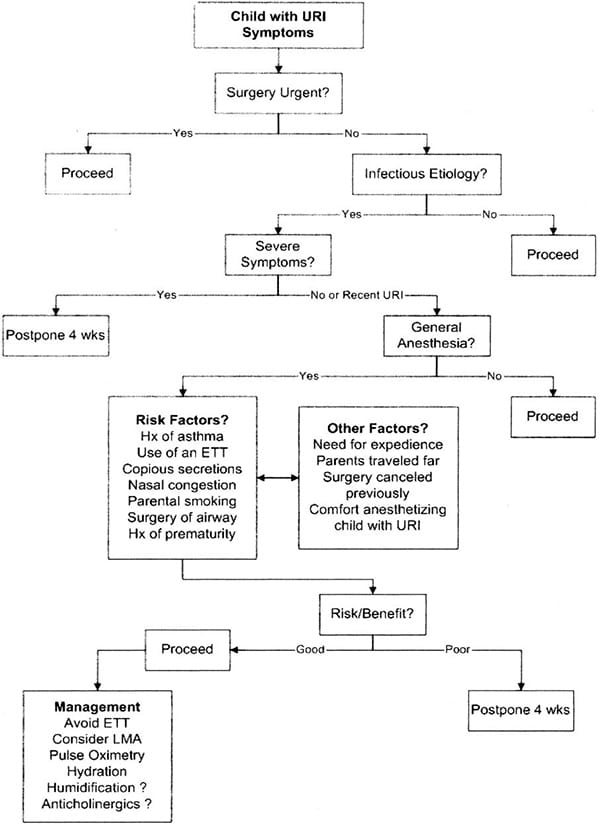
Figure 5. algorithm for the assessment and anesthetic management of the child with an upper respiratory infection. URI = upper respiratory infection; Hx = history; ETT = endotracheal tube; LMA = laryngeal mask airway.
Mild symptoms of URI constitute – clear runny nose, sneezing, onset not acute, overall active, age > 1 year
More severe symptoms – croupy cough, fever ≥ 38 c, presence of malaise, lethargy, loss of appetite as confirmed by parents, symptoms and signs of LRI such as wheezing and rales, associated poorly controlled reactive airway disease, especially in a child < 6 -12 months of age
Children presenting for elective procedures with symptoms of a URI require careful preoperative assessmentl. The lungs should be auscultated to exclude any lower respiratory
tract involvement, and a chest radiograph should be considered if the examination is questionable. Chest radiograph findings typically lag behind the presentation of clinical symptoms in children with lower respiratory infections.
In general, children presenting with symptoms of an uncomplicated URI and who are afebrile with clear secretions and appear otherwise healthy, or those with noninfectious conditions, should be able to undergo surgery. Rolf and Coté (29) suggest that “children with a mild URI may be safely anesthetized, since the problems encountered are generally easily treated and without long-term sequelae.” Children with more severe symptoms—including mucopurulent secretions, productive cough, fever >38°C, lethargy, or signs of pulmonary involvement—should have their elective surgery postponed for a minimum of 4 wk. Similarly, if a bacterial infection is suspected, patients should be placed on antibiotic therapy, and their surgery should be postponed for ≥4 wk.
Anesthesia Management
Viral infection make the airway sensitive to secretions, potentially irritant anesthetic gases, or airway manipulation. Management of the child with a URI is directed at minimizing secretions and avoiding stimulation of a potentially sensitive airway.
The use of anticholinergics such as glycopyrrolate or atropine may be useful in reducing secretions and attenuating vagally-mediated hyperreactivity.
Bronchodilator premedication has also been suggested as a means to reduce autonomically mediated airway complications. However, in one study, Elwood et al. (30) showed that premedication with either albuterol or ipratropium had no effect on URI-related respiratory complications. However, Silvanus et al. (31) showed that in adult patients with bronchial hyperreactivity, preoperative treatment with combined corticosteroids and salbutamol minimized intubation-evoked bronchoconstriction more effectively than inhaled salbutamol alone. In one recent observational prospective pilot study it was concluded that premedication with salbuterol in children with URI decreases the incidence of bronchospasm and coughing.(32)
Use of an ETT should be avoided if possible, because its use, particularly in young children, significantly increases the risk of airway complications. The LMA, however, has been shown to provide a safe alternative for some procedures in which an ETT might otherwise be used. One study showed that the LMA is associated with fewer episodes of respiratory complications, including bronchospasm and arterial oxygen desaturation.(33)
In the past, halothane was considered the volatile anesthetic of choice in these children. However, sevoflurane results in fewer complications than halothane particularly when sevoflurane is used for both induction and maintenance. Thiopentone is associated with the highest incidence of adverse events, sevoflurane and propofol with the lowest. Ketamine produces bronchodilation, but may not be indicated because it will further increase airway secretions.
Unnecessary stimulation without adequate depth of anesthesia during induction should be avoided. Regardless of the induction drug used, it is imperative that the depth of anesthesia be sufficient to obtund the airway reflexes, particularly when an ETT is placed. Direct spraying of the airway may trigger an airway reaction therefore, the i.v. route ( Lignocaine 1 – 1.5 mg/Kg, 1-3 min before intubation) is preferable.(32)
The optimal depth of anesthesia at which tracheal extubation should occur is less clear. There is no consensus on the optimum depth of anaesthesia at which extubation of the trachea or removal of the LMA should be done. Many anaesthetists would prefer to remove the airway when the patient is awake to enable the patient to clear secretions and better protect the airway. . Although some prefer to extubate under deep anesthesia to avoid reflex constriction of the airways. Adverse respiratory events were found to be more in children with URI when they were premedicated with midazolam and/or were extubated deeply. Preoperative sedation may lower postoperative minute ventilation due to residual sedation, making the patient more prone to desaturation (32)
Suctioning of excess secretions is important in preventing mucus from plugging bronchus or ETT. Suctioning of airway should be done under deep anesthesia.
Humidification may also be important in children with URIs, particularly for long cases. Humidification may help to minimize drying and inspissation of secretions by anesthetic and carrier gases and may maintain adequate ciliary clearance mechanisms.
Supplemental oxygen should be administered to patients with URI who are prone to desaturate postoperatively. On the basis of best evidence available at the present time, a child with mild uncomplicated URI undergoing minor surgical procedures can be safely anesthetized without any increase in risk. Child with severe symptoms should have surgery postponed for at least 4 wk. The dilemma therefore arises with an otherwise healthy child whose symptoms lie between these extremes, who has associated risk factors, or who is asymptomatic but has a recent history of URI. Decisions regarding the suitability of proceeding with anesthesia for these children must be considered on a case-by-case basis, bearing in mind the presence of identified risk factors (e.g., reactive airway disease, ETT use, type of surgery, and presence of nasal congestion and sputum), the need for expedient surgery, and the anesthesiologists’ experience and comfort with anesthetizing the child with a URI. Consideration of these elements, together with a tincture of common sense and good judgment, is critical as a means to assess the individual risk/benefit profiles, identify and prepare for potential complications, and optimize the anesthetic management accordingly. (27)
REFERENCES:
- Tierney WM, Murray MD, Gaskins DL, Zhou XH. Using computer-based medical records to predict mortality for inner-city patients with reactive airways disease. J Am Med Informatics Assoc 1997;4:313–321. [CrossRef] [Medline]
- Moudgil GC. The patient with reactive airways disease. Can J Anaesth 1997;44:R77–R83. [CrossRef] [Medline])
- JOHN V. FAHY and PAUL M. O’BYRNE "“Reactive Airways Disease”", American Journal of Respiratory and Critical Care Medicine, Vol. 163, No. 4 (2001), pp. 822-823. )
- www.iars.org/2002.ReviewCourseLectures/pdfs/gal2002.pdf
- Warner DO, Warner MA, Barnes RD, et al. Perioperative respiratory complications in patients with asthma. Anesthesiology 1996;85:460 –7.
- Little JW, Wall WJ, Douglass RG, et al. Airway hyperactivity and peripheral airway dysfunction in influenza infection. Am
Rev Respir Dis 1978;118:295–303 - Burburan SM, Xisto DG, et al. Anaesthetic management in asthma.. MINERVA ANESTESIOL 2007;73:357-65
- Pearce AC, Jones RM. Smoking and anesthesia: preoperative abstinence and postoperative morbidity. Anesthesiology 1984; 61:576–84.
- Erskine RJ, Murphy PJ, Langton JA. Sensitivity of upper airway reflexes in cigarette smokers: effect of abstinence. Br J Anaesth 1994;73:298 –302.
- Salmeron S, Bronchard L, Mal H, et al. Nebulized versus intravenous albuterol in hypercapnic acute asthma. Am J Respir Crit Care Med 1994;149:1466 –70.
- Littenberg B. Aminophylline treatment of severe acute asthma: a meta analysis. JAMA 1988;259:1678–84.
- Kabalin CS, Yarnold PR, Grammer LC. Low complication rate of corticosteroid-treated asthmatics undergoing surgical procedures. Arch Intern Med 1995;155: 1379-84.)
- Gal TJ, Surratt PM. Glycopyrrolate and atropine inhalation: comparative effects on normal airway function. Am Rev Respir Dis 1984;129:871–3.
- Gal TJ, Surratt PM. Atropine and glycopyrrolate effects on lung mechanics in normal man. Anesth Analg 1980;60:85–90.
- Wu RSK, Wu KC, Wong TKM. Effects of fenoterol and ipratropium on respiratory response of asthmatics after tracheal intubation. Br J Anaesth 2000;84:358–62.
- Brichant JF, Gunst SJ, Warner DO, Rehder K. Halothane, enflurane and isoflurane depress the peripheral vagal motor pathway in isolated canine tracheal smooth muscle. Anesthesiology 1991;74:325–32.
- Brown RH, Zerhouni EA, Hirschman CA. Comparison of low concentrations of halothane and isoflurane as broncho-dilators. Anesthesiology 1993;78:1097–101.
- Rook GA, Choi JH, Bishop MJ. The effect of isoflurane, halothane, sevoflurane, and thiopental nitrous oxide on respiratory
system resistance after tracheal intubation. Anesthesiology 1997;86:1294 –9. - Goff MJ, Shahbaz RA, Ficke DJ, et al. Absence of bronchodilation during desflurane anesthesia. Anesthesiology 2000;93: 404–8.)
- Pizov R, Brown RH, Weiss YS, Baranov D, Hennes H, Baker S et al. Wheezing during induction of general anesthesia in patients with and without asthma. A randomized, blinded trial. Anesthesiology 1995;82:111-6.
- Eames WO, Rook GA, Wu RSC, Bishop MJ. Comparison of the effects of etomidate, propofol, and thiopental on respiratory resistance after tracheal intubation. Anesthesiology 1996;84: 1307–11.)
- Bulut Y, Hirschman CA, Brown RH. Prevention of lidocaine aerosol-induced bronchoconstriction with intravenous lidocaine. Anesthesiology 1996;85:853–9.)
- Groeben H, Schwelen A, Irsfeld S, et al. High thoracic epidural anesthesia does not alter airway resistance and attenuates the response to an inhalational provocation test in patients with bronchial hyperreactivity. Anesthesiology 1994;81:868 –74.
- Olsson GL. Bronchospasm during anaesthesia. A computer-aided incidence study of 136,929 patients. Acta Anaesthesiol Scand 1987; 31: 244-52.
- Update in Anaesthesia | www.anaesthesiologists.org
- Tait AR, Malviya S, Voepel-Lewis T, et al. Risk factors for perioperative adverse respiratory events in children with upper respiratory tract infections. Anesthesiology2001; 95: 299–306.
- Tait AR, Malviya S, Anesthesia for the Child with an Upper Respiratory Tract Infection: Still a Dilemma? Anesthesia & Analgesia2005; 100: 59 – 65.
- Parnis SJ, Barker DS, Van Der Walt JH. Clinical predictors of anaesthetic complications in children with respiratory tract infections. Paediatr Anaesth2001; 11: 29–40.
- Rolf N, Coté CJ. Frequency and severity of desaturation events during general anesthesia in children with and without upper respiratory infections. J Clin Anesth1992; 4: 200–3.
- Elwood T, Morris W, Martin L, et al. Bronchodilator premedication does not decrease respiratory adverse events in pediatric general anesthesia. Can J Anaesth2003; 50: 277–84.
- Silvanus M-T, Groeben H, Peters J. Corticosteroids and inhaled salbutamol in patients with reversible airway obstruction markedly decrease the incidence of bronchospasm after tracheal intubation. Anesthesiology2004; 100: 1052–7.
- Sallman B,The Child with a Recent URI Curr Rev Clin Anesth 32 (14): 161-172)
- Tait AR, Pandit UA, Voepel-Lewis T, et al. Use of the laryngeal mask airway in children with upper respiratory tract infections: a comparison with endotracheal intubation. Anesth Analg1998; 86: 706–11.





