
MANAGEMENT OF POSTOPERATIVE RIGHT VENTRICULAR DYSFUNCTION IN A PATIENT OPERATED FOR AORTIC VALVE REPLACEMENT SURGERY FOR SEVERE CALCIFIC AORTIC STENOSIS IN THE CONGENITAL BICUSPID AORTIC VALVE
DR RITESH BORKAR
Consultant Cardiac Anesthesiologist,
Viveka Hospitals, Nagpur
Introduction: Bicuspid aortic valve is a congenital heart disease. Usually the patients are asymptomatic unless they develop aortic regurgitation or stenosis leading to symptoms. Therapeutic intervention is decided according to the Severity of disease.
Recently we operated upon a patient having Bicuspid aortic valve with severe calcific aortic stenosis in our Institute.
Case : 55years, Male, presented with H/O dyspnoea on exertion since 2-3 years on and off. Known case of Hypertension and Aortic Stenosis. Advised AVR in past but didn’t comply.
On clinical Examination: Weight: 65.1 Kg Height: 167cm BSA: 1.74m2
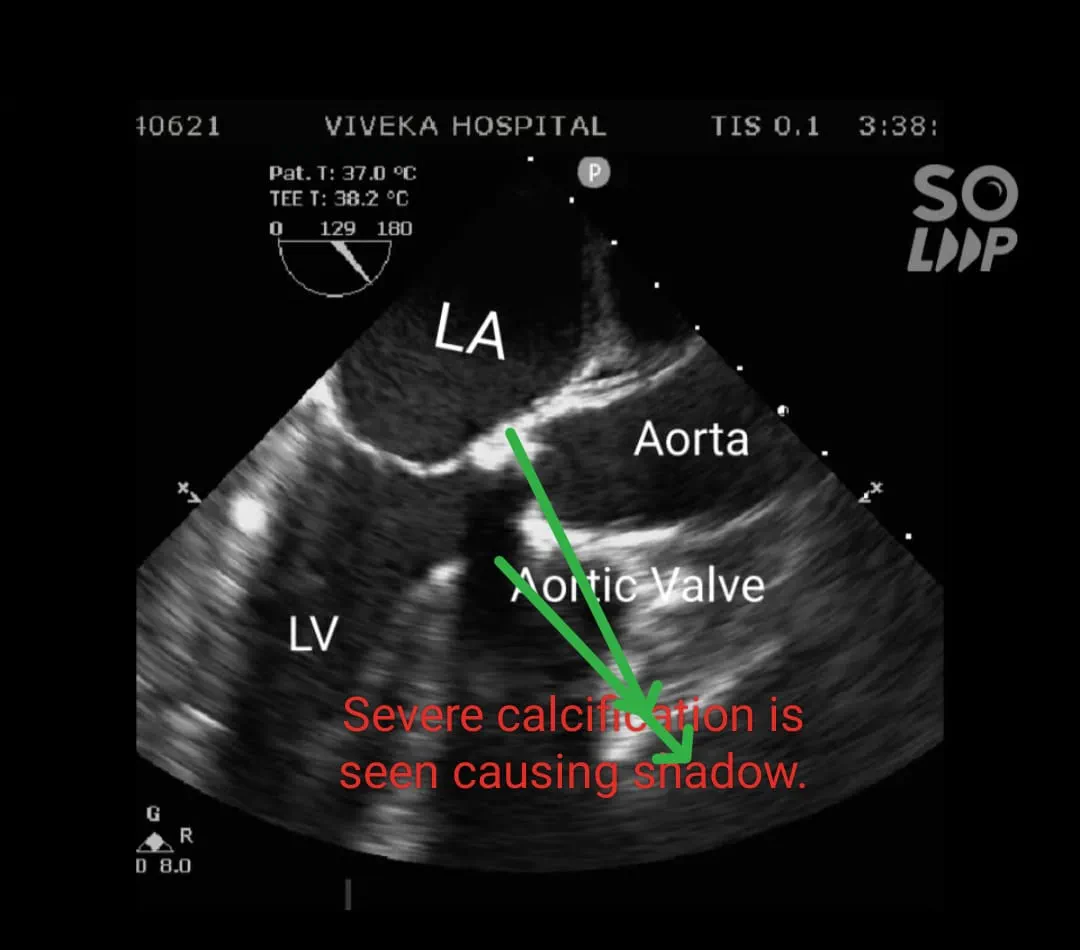
He was found to have restricted mouth opening due to submucosal fibrosis due to tobacco chewing. Vitals were normal. On auscultation he had an ejection systolic murmur conducted to the carotids. Other systemic examination was within normal limits. ECG showed Left ventricular strain. 2D ECHO revealed Severe calcific AS in a bisuspid Aortic valve with a gradient of 137/77 mm of Hg. Severe Concentric Left ventricular hypertrophy (LVH) No RWMA. EF 65%.
Other valves were normal. Coronary Angiography was normal.
CT Chest : Severe calcific aortic valve with calcification in Ascending Aorta and arch of aorta.

After complete investigations the patient was posted for Aortic Valve Replacement surgery.
Informed Consent was obtained. NBM for 8 hours before surgery.
Medications before Surgery : Tab. Pantoptazole 40mg,Diuretic and a Betablocker were continued.
Taken in OR, routine monitoring : ECG,SpO2 ,NIBP, Temperature and ETCO2.
Invasive Lines : Under Local Anaesthesia Right Radial artery cannulated with 20 G arterial cannula. Right femoral artery was cannulated with 16 G arterial cannula. Right Internal Jugular vein was 8Fr 4 lumen catheter.
Premedication : IV Midazolam 2 mg and IV Fentanyl 150micg in elliquots.
General Anaesthesia was administered using IV Etomidate 20 mg and inhaled Sevoflurane. Check Laryngoscopy was performed before administering SMR and was found that intubation could be accomplished. Cormack Lehane 3.
IV succinyl Choline was administered and trachea intubated with ETT No. 8.5. Air entry confirmed and ETT fixed.
Maintenance: O2 + Air+ Isoflurane + IV Vecoronium 0.2mg/Kg and intermittent doses + Intermittent doses of IV Fentanyl and IV Midazolam+ IV Propofol boluses as and when required.
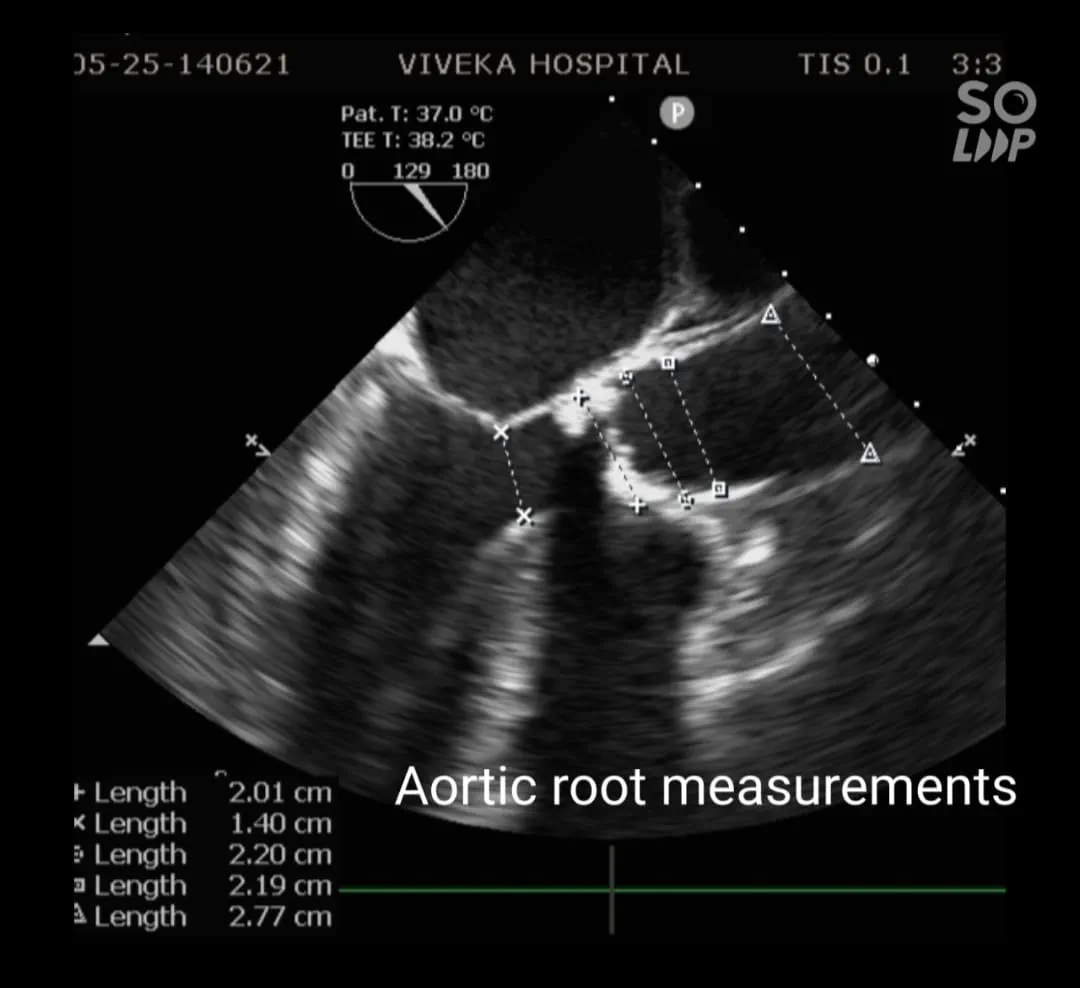
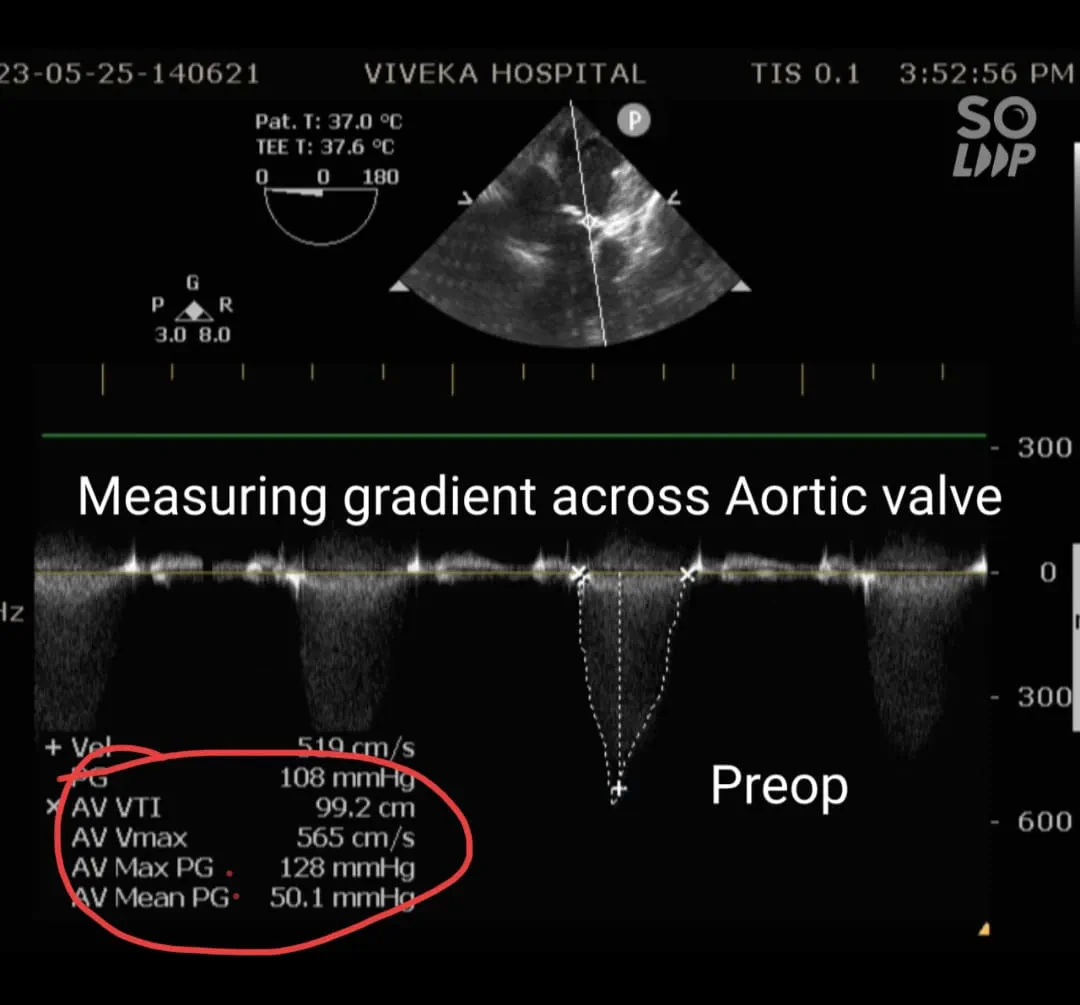
Transoesophageal echocardiography: Findings of Transthoracic ECHO confirmed. Aortic annulus : 20.1mm
Gradient : 128/50 mm of Hg. Mild Aortic regurgitation. Severe Concentric Left ventricular hypertrophy. Calcific Aortic Valve with area 0.349 cm2.
After Painting and draping surgery was started. After sternotomy pericardiotomy was done and heart exposed. Patient was administered IV Heparin 3mg/Kg.
After 3 min cannulation done.
Ascending Aorta : 22 Fr
RA : Dual stage 36/46Fr
Activated Clotting Time(ACT) was 482 sec. Cardiopulmonary bypass was initiated and mechanical ventilation was stopped.
On CPB Anaesthesia management : IV Midazolam 3 mg + Inj. Fentanyl 150 micg + Inj. Vecuronium infusion @ 3 mg/hour.
Aorta crossclamped,antegrade and retrograde cardioplegia given for myocardial protection.
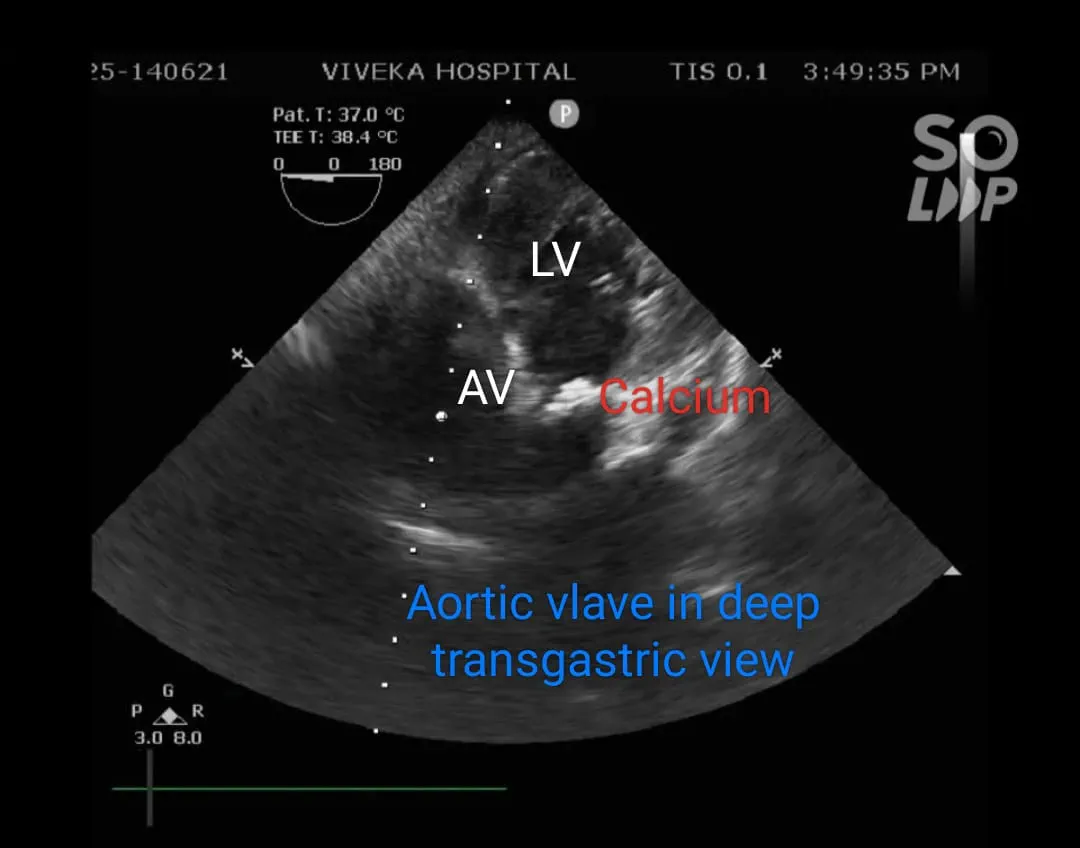
Findings after opening aorta: Aortic Valve was bicuspid and heavily calcified. Indigenous aortic valve excised and calcium debrided.
21 mm bioprosthetic valve( Daffodil) was used for replacement.
Aortic Crossclamp time : 66 minutes
After aortic closure, heart was de aired and Crossclamp released.
Ventilation restarted.
Cardiac activity returned on minimal inotropic supports Adrenaline and Noradrenaline.
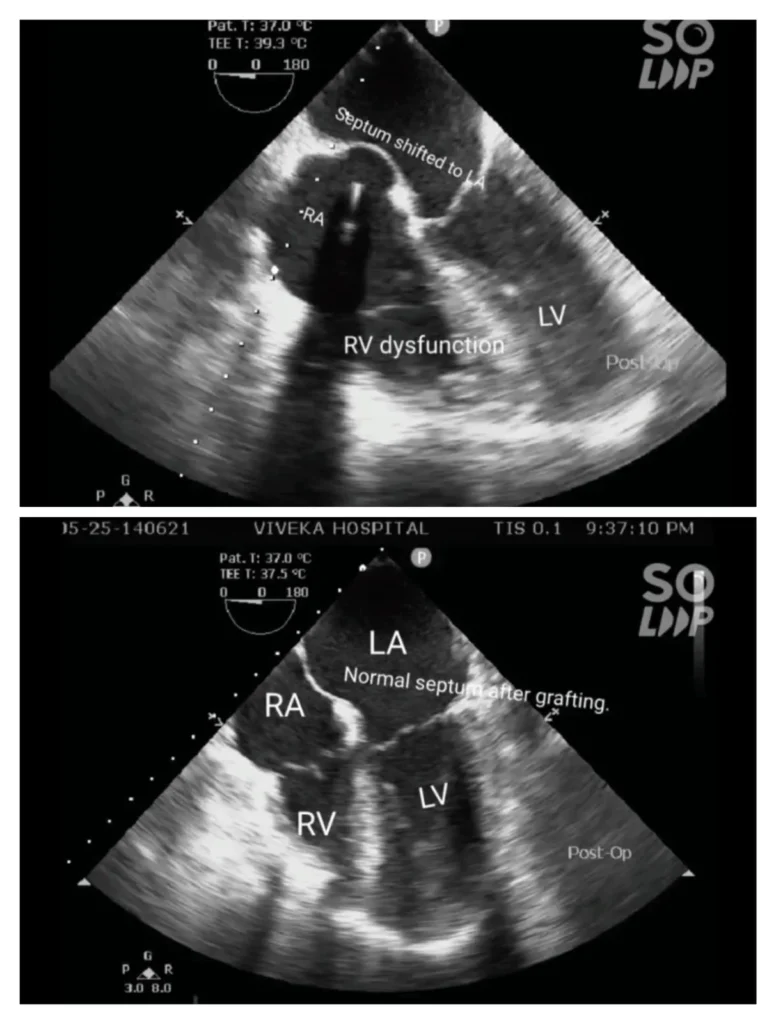
After adequate rest time, gradually patient was weaned off cardiopulmonary bypass. RV distension noted. On TEE gross RV dysfunction was found with increase in RA pressure pushing the atrial septum into the LA. Inotropic supports increased and Milrinone started.

Prosthetic Aortic Valve was functioning well.
The patient had hypotension and bradyarrhythmias. Temporary Pacing was done after placing the Epicardial pacing wires. Hypotension was not responding to conventional therapy of inotropes and inodilators. Hence was taken back on full cardiopulmonary bypass.
After extra rest time the CPB was weaned off. But again the patient developed RV dysfunction after sonetime and we had to go back on CPB. Another couple of attempts failed.
We suspected the possibility of embolism of calcified material in the RV branch of RCA(Right Coronary Artery).
Finally a saphenous vein graft from left leg was harvested and interposed between RV branch and the Ascending Aorta. Another attempt to wean off CPB and this time the RV function was normal.
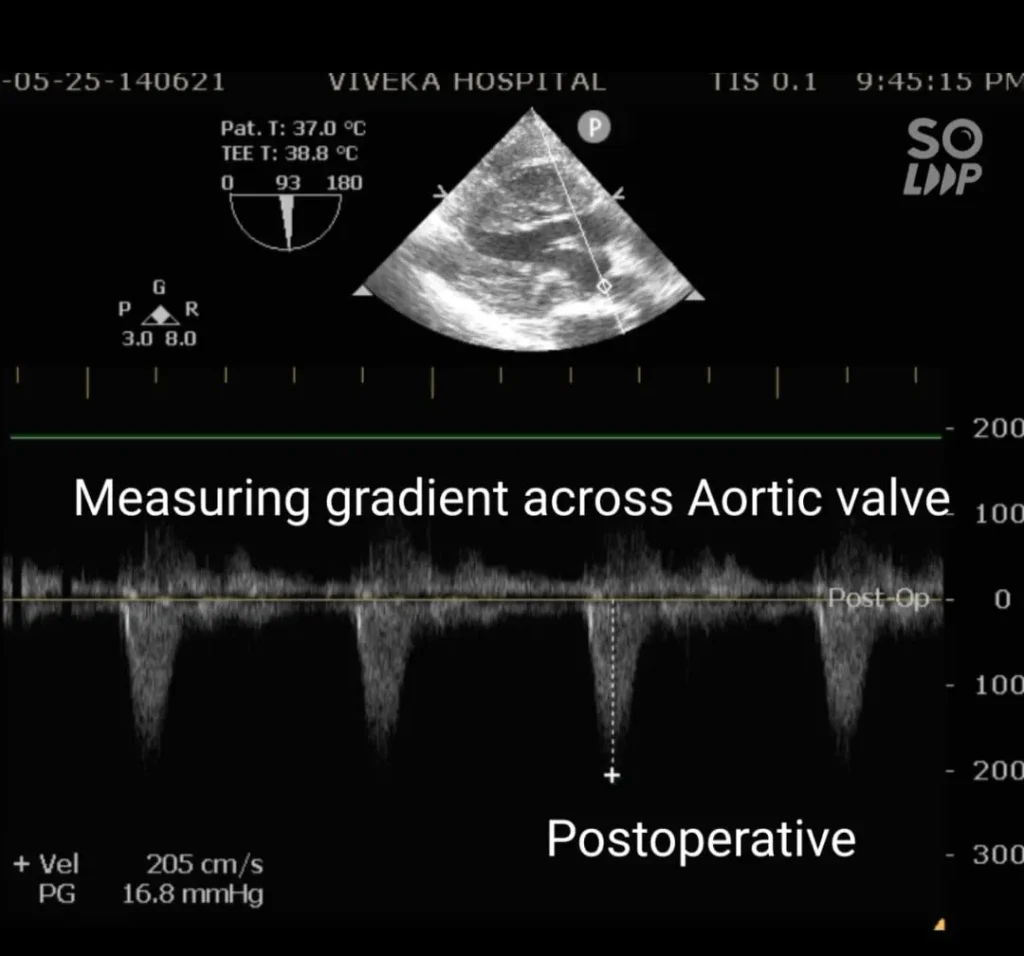
TEE showed that the prosthetic Aortic Valve was functioning well with a peak gradient of 16.2mmHg.
Additional doses of IV Midazolam 2 mg and Fentanyl 150 micg alongwith IV Vecuronium infusion @3 mg/hr continued throughout the CPB till closure.
CPB Times : 2 hr 20 min, 40 min & 24 min
After closure the patient was shifted to surgical ICU(SICU) on moderate dose of Adrenaline,Milrinone and Noradrenaline on manual ventilation.
In SICU patient was ventilated overnight and sedated using IV Midazolam + Fentanyl infusion and Cisatracurium infusion. Postoperative objectives were to maintain the mean BP above 70 mm Hg and urine output 1.5 – 2 ml/Kg/Hr. Avoid hypertension.
Patient was stable and maintained adequate urine output, hence was gradually weaned of the ventilator and extubated next morning. Rest of the stay in SICU was uneventful. His vasopressor and inotropic supports could be gradually tapered of in next 2 days.
His Drains and invasive Lines were removed and was mobilized out of bed.
He was shifted to ward room on day 3. In ward his stay was uneventful. He was subjected to 2D ECHO screening and the prosthetic Aortic Valve was found to be functioning well. There was no RV dysfunction. He was discharged on Day 8 in stable condition.






Discussion: Approximately 2% of the population has Bicuspid AV. The cause is probably genetic and is likely to be hereditary. There are almost 25 percent chances of having Bicuspid AV in first-degree relatives of patients diagnosed with Bicuspid AV. Bicuspid AV shows male preponderance. Patients with Turner syndrome may have Bicuspid AV.
About 1 in 3 patients with a bicuspid aortic valve develop complications like stenosis and/or regurgitation with aging.
These patients are at increased risk of developing aortic aneurysm and dissection. At the tissue level, the aorta shows cystic medial necrosis, loss of elastic fibers, increased apoptosis, and altered smooth muscle cell alignment. Patients with a bicuspid valve have larger aortic root dimensions and an increased rate of aortic dilation over time. The risk of aortic dissection in patients with a bicuspid valve is 5 to 9 times higher than in the general population.
About 15% to 20% of bicuspid valve patients have incomplete valve closure causing aortic regurgitation and present at age 20 to 40 years.
The majority of patients with a bicuspid valve have relatively normal valve function and remain undiagnosed until late in adulthood, when stenosis develops because of superimposed leaflet calcification. The cellular and molecular mechanisms involved in the calcification of a bicuspid aortic valve appear to be similar to the process in a trileaflet valve. Aortic leaflet calcification starts as a focal area on the aortic side of the leaflet with subendothelial accumulation of lipoproteins and an inflammatory cell infiltrate. There is lipoprotein oxidation with infiltration of macrophages and T lymphocytes and local production of proteins associated with inflammation and tissue calcification. This leads to increased leaflet stiffness with a reduction in systolic valve opening. When patients present with symptoms resulting from valve obstruction, the treatment is valve replacement.
Roberts and Ko reported that the prevalence of bicuspid aortic valve was 53% in a consecutive series of 933 patients undergoing valve replacement for isolated aortic stenosis. The 3 most common causes of aortic stenosis are :
- Bicuspid valve
- Rheumatic disease
- Calcification of a trileaflet valve( aging).
- In a cohort study by David Levy et al, the authours found that around 2.9% patients undergoing cardiac surgeries develop RV dysfunction. In the postoperative period.
- The risk factors for postoperative RV dysfunction are :
- Old age
- Preoperative AF
- LVEF less than 50%
- Pulmaonary Hypertension(PASP more than 55 mm of Hg).
- High EURO Score preop.
- The patients undergoing Mitral and Tricuspid valve surgery are at more risk of developing RV dysfunction.
- Mechanisms of RV dysfunction include :
- Suboptimal myocardial protection.
- Prolonged CPB time
- RV ischaemia/ infarct
- Postoperative Pulmonary embolism
- Atrial arrhythmias and atrioventricular dys synchrony
- Pre existing Pulmonary artery disease.
- Reperfusion Lung injury after CPB
- Protamine induced Pulmonary Hypertension.
- Increased PVR due to atelectasis of lungs during CPB.
- Our patient didn’t have any of the risk factors. RV ischaemia due to embolism of calcific material in the RV branch is probably the cause of RV dysfunction in our patient and this was treated with the grafting.
- The management of RV dysfunction :
- Pulmonary vasodilators : NTG,Milrinone, inhaled Nitric Oxide, Sildenafil.
- Optimal IV fluid management
- Diuretics: Frusemide,Torsemide
- Inotropes : Adrenaline and Noradrenaline
- Vasopressors : Noradrenaline
- Inodilators : Dobutamine,A mrinone, Milrinone
Restoration of RV myocardial perfusion pressures by grafting or stenting. This was done in our patient and he responded well.
Conclusion: Bicuspid Aortic valve is a congenital heart disease, usually asymptomatic in early age. Aortic regurgitation may develop between 20-40 years age. Stenosis and calcification develop later. Aortic Valve Replacement and Trancatheter Aortic Valve Replacement are the treatment modalities available depending upon the severity of calcification.
Post cardiopulmonary RV dysfunction is a known phenomenon and occurs in 2.9% of patients undergoing cardiac surgeries. It can be treated using the pulmonary vasodilators and inodilators. RV dysfunction increases duration of elective ventilation, ICU stay ,hospital stay and overall morbidity and mortality, But the mortality andorbidity are comparable to other Cardiac surgical patients who don’t develop RV dysfunction.




