
Prof and HOD Dept.of Anaesthesiology,
NKPSIMS
INTRODUCTION:
Alteration in body temperature is common during anaesthesia. In human beings, body temperature is maintained within a very narrow range by way of afferent sensing, central processing and efferent thermoregulatory responses(fig 1)1. All these components of the thermoregulatory system are impaired by anaesthesia.
The role of anaesthesiologist is to maintain physiologic homeostasis during the perioperative period, during which anaesthesia and surgery create an abnormal physiologic state and hence the need to monitor body temperature along with other vital signs and efforts should be made to maintain normothermia.
BODY THERMOREGULATION:
The anterior hypothalamus is the centre of thermoregulatory control2. The relative contribution of thermal information to the central the thermoregulatory system is 80% from the core and deep body tissue and 20% from skin surface3. This information is compared in hypothalamus to an internal set point temperature which is analogous to the setting on a thermostat. When body temperature is above or below this set point, the first response is behavioural that involves changing the ambient temperature or altering ones clothing. When behavioural thermoregulation is inadequate and temperature exceeds the setpoint, vasodilation and sweating triggers the heat release and when the temperature is below the set point, vasoconstriction is triggered to conserve heat and shivering to produce heat.
The efferent thermoregulatory responses comprise of threshold, gain and maximum intensity4. These are important concepts because they are used to quantitatively assess the degree of thermoregulatory impairment with various anaesthetics as well as the differences in thermoregulation between various individuals.
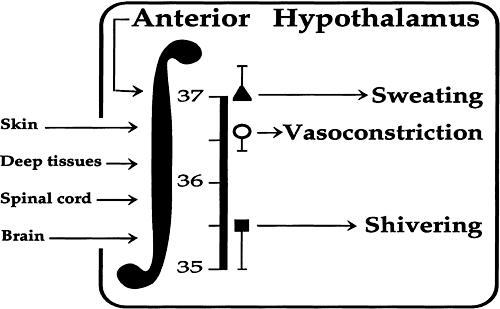
Figure 1. Afferent input of thermal information is derived from tissues throughout body. A mean body temperature below the set point initiates cold responses(vasoconstriction, shivering and nonshivering thermogenesis). A mean body temperature above the set point triggers warm responsesvasodilation and sweating).(From Sessler DI: N Engl J Med 336:1730, 1997.)
BODY TEMPERATURE MONITORING:
Body has two thermal compartments: the core and the periphery5. The core has a fairly constant internal temperature that is protected by the insulation from the peripheral compartment. Normal core temperature lies within the range of 36.5° to 37.5° C. Chest, abdomen, pelvis and head make up the core compartment whereas extremities and skin make up the peripheral compartment.
The best monitoring sites which are closest to blood temperature is the true core temperature. These sites are in order of greatest to least correlation with core temperature: pulmonary artery, distal 1/3rd oesophagus, tympanic membrane, nasopharynx, oral/ sublingual cavity, urinary bladder, rectum and skin surface6.
ANAESTHSIA AND TEMPERATURE REGULATION:
Anaesthetics can modify heat balance by altering one or more of the 3 compartments: the afferent pathway, central control or efferent pathway. General anaesthesia impair all three compartments whereas regional anaesthesia impairs afferent and efferent pathway.
The interthreshold range is a range of temperatures that do not trigger a response. This range (between sweating and vasoconstriction) is normally only a few tenths of a degree centrigrade (0.2°C)7, which is expanded approximately ten folds by anaesthesia. This effect of anaesthesia renders patients poikilothermic 1,4 and body temperature drifts towards environmental temperatures.
FEVER:
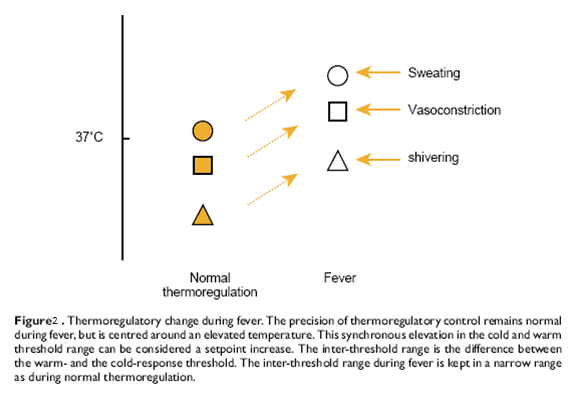
Fever is a regulated increase in body temperature where the set point increases and heat loss and heat production are regulated to higher temperature (fig 2)7, 8.
Passive hyperthermia is also an increase in body temperature in which the thermoregulatory set point is normal. Here the heat production by the body exceeds the heat loss.
During general anaesthesia, most patients become hypothermic. However, hyperthermia occurs at relatively higher incidence during anaesthesia in paediatric patients, in patients with brain stroke or injury or acute peritonitis or in otolargyngeal surgeries.
Differentiation between passive hyperthermia and fever under general anaesthesia is difficult, however with fever patient will have vasoconstriction and shivering at emergence.
Fever is considered as a protective response to infection8. The host survival rate, as observed in few studies8 has improved with increases in body temperature and the use of antipyretics significantly decreased the host survival rate. Although fever may be beneficial for infected patients, the associated symptoms, such as increasing cardiac output, oxygen consumption, and energy consumption, are sometimes harmful. In such cases, antipyretic use needs to be considered.
Fever is mediated by immune, endocrine and neuronal systems8. Fever is induced by endogenous pyrogens and probably by vagal signals.
During the perioperative period, external factors such as anaesthesia, sedatives, surgical procedures and perioperative examinations modulate fever.
THERMAL MANAGEMENT GUIDELINES9
To detect thermal disturbances and maintain appropriate body temperature during anaesthesia.
- Core body temperature should be measured in most patients given general anaesthesia for more than 30 mins.
- Temperature should also be measured in regional anaesthesia when change in body temperature are intended, anticipated or suspected.
- Unless hypothermia is indicated, effort should be made to maintain intraoperative core temperature higher than 36°C.
GENERAL ANAESTHESIA and FEVER
Volatile anaesthetics, propofol, opioids and sedatives all slightly increase the sweating threshold while markedly decreasing the vasoconstriction and shivering thresholds8. As a result, the sweating-to-vasoconstriction inter-threshold range, which is usually only a few tenths of a degree centigrade (°C), increases to a 2–4°C range, depending on the drug and dose8.
- Volatile anaesthetics.
The mechanism by which volatile anaesthetics inhibit fever include:
primarily central action of volatile anaesthetics8 and peripherally mediated inhibition via reduced release of pyrogenic cytokines8. - Intravenous anaesthetics.
Anaesthetics increase the sweating threshold and markedly decrease the vasoconstriction and shivering thresholds, and thus increase the inter-threshold range8.
However in fever, there is regulated increase in the thermoregulatory thresholds, but does not decrease the precision of thermoregulatory control.
The combination of general anaesthesia and fever simply produces an expanded interthreshold range around the elevated setpoint. Hence, the decrease in thermoregulatory thresholds of cold defences will diminish fever in the cold environment of operating rooms. - Opioids.
Opioids also increase the interthreshold range like volatile & IV anaesthestics. Thus they also attenuate fever in a dose dependent manner. Thus need to be aware of opioid use in intensive care units or during the post-operative period because opioids can attenuate fever, which is an important symptom of infection.
Opioids are immunosuppressive8, which is also dose dependant hence large doses should be used with caution. - Skeletal muscle relaxant.
At the start of fever, vasoconstriction and shivering play the important role of increasing body temperature. Paralysis prevents shivering and the associated increase in metabolic heat production, leaving the development of fever entirely dependent on thermoregulatory vasoconstriction. Therefore, alteration of vasomotor tone by general anaesthesia is one of the primary factors that influences intraoperative core temperature8. Paralysis slightly reduces the magnitude of fever by preventing shivering, although its effect seems to be less important than anaesthetic-induced inhibition of fever.
NEUROAXIAL ANAESTHESIA
Re-distribution is a major cause of core hypothermia during epidural and spinal analgesia, contributes to 89% initially8. Core temperature decreases 0.8 – 0.3°C in the first hour of epidural or spinal anaesthesia which is half compared to general anaesthesia. Peripheral nerve block is a more important cause of hypothermia. Shivering and vasoconstriction occur after sufficient core hypothermia but only in the unblocked areas which is insufficient to prevent further hypothermia. Thus nueroaxial blockade will also attenuate fever.
EPIDURAL ANAESTHESIA
Several studies demonstrate that average temperature is higher in patients given epidural analgesia for labour or post-operative pain treatment8.
With epidural anaesthesia, sweating threshold increases slightly and sweating is reduced in blocked areas. When metabolic rate increases as in labour, heat production exceeds heat loss. Here, epidural analgesia is assumed to cause passive hyperthermia8.
However, in postoperative period these patients have normal metabolic rates and ICU environment is not warm enough to induce passive hyperthermia. Inflammatory cytokines are increased during the post-operative period which may attribute towards fever with epidural analgesia8.
POSTOPERATIVE FEVER
It is common and may be a normal inflammatory response induced by surgical stress, and not always infection. Many drugs used in post operative period like opioid, sedatives and NSAIDs may modulate postoperative fever. Fever is considered the earliest and most easily detected sign of infection in surgical patient and hence core body te `peratures should be measured in early postoperative period.
Fever workups should be done only in high risk patients as it is not cost effective and fever in postoperative period is mostly due to surgical stress. Plasma IL6 concentration are found to be a good predictor for infection8.
TREATMENT OF FEVER
Fever should be treated with antipyretics in patients with cardiopulmonary dysfunction, acute brain stroke or injury, or in whom temperature exceeds 40°C. Active cooling is effective for sedated and paralysed patients but not in awake patients as it provokes thermal discomfort.
MALIGNANT HYPERTHERMIA10
This Neuromuscular disorder occurs after exposure to triggering agents like inhalational agents and succinylcholine. Incidence is 1:12000 to 1:40000. It is inherited by autosomal dominant pattern with mixed penetrance. Multiple mutations for the ryanodyne receptor of the sarcoplasmic reticulum are causative. Triggering agents cause an imbalance between release and reuptake of calcium from sites of sarcoplasmic reticulum. The resulting increase in intracellular calcium favours contraction and limits relaxation.
Clinical presentation can be immediate or delayed upto 24 hours after exposure to inhalational agents or succinylcholine. It includes rise in ETCO2 (initial sign), metabolic acidosis, tachycardia, hypertension, cardiac dysarrythmias, core temperature elevation exceeding 43°C (late sign). Elevated serum potassium, CPK, myoglobin and ionized calcium is also seen.
Confirmation of MH requires detection of myoglobin in urine. Skeletal muscle biopsy is the gold standard of MH diagnosis. Thyroid strom, pheochromocytoma and neurolept malignant syndrome needs to be ruled out.
Treatment
- Discontinue the triggering agent.
- Dantrolene 2.5 mg/kg iv repeated every 5 mins until tachycardia, muscle rigidity, ETCO2 and fever are controlled. It is avoided in pregnant patients.
- Hyperventilation with 100% O2
- Administer sodabicarb 1-2 mEq/kg according to ABG.
- Cooling the patient: ice packing, irrigation of body cavities and infuse cold IV fluids.
- If no response to acidosis and hyperkalemia, administer antiarrhythmics.
- Calcium channel blockers are contraindicated.
- Manage hyperkalemia: hyperventilation, sodabicarb, insulin and glucose and calcium.
- Maintain urine output 2ml/kg/hr.
REFERENCES:
- Sessler DI. Mild perioperative hypothermia. N Engl J Med 1997, 336: 1730.
- Benzinger TH. Heat regulation: hemostasis of central temperature in men. Physiol Rev 1969, 49: 671.
- Cheng C, Matsukawa T, essler DI et al. Increasing mean skin temperature linearly reduces the core temperaSture thresholds for vasoconstriction and shivering in humans. Anesthesiology 1995, 82:1160.
- Sessler DI. Perianesthetic thermoregulation and heat balance in humans. FASEBJ 1993, 7: 638.
- DuBois EF. The many different temperatures of the human body and its parts. West J Surgery Obstet Gynecol 1951, 59:476.
- Cork RC, Vaughan RW, Humphrey LS. Precision and accuracy of intraoperative temperature monitoring. Anesth Analg 1983, 62:211.
- Lopez m, Sessler Di, Walter K, et al. Rate and gender dependence of the sweating vasoconstriction, and shivering thresholds in humans. Anesthesiology 1994, 80:780.
- Negishi C, Lenhardth R. Fever during anesthesia. Best practice & Research Clinical Anesthesiology 2003, 17(4): 499-517
- Miller RD, Eriksson LI, Fleisher LA, et al. Miller’s Anesthesia 7th edition. Churchill Livingston Elsevier 2010, vol 1: 1551.
- Reed A.Francine S.Yudkonitz. Clinical cases in anesthesia.3rd Edition.Elsevier Churchill Livingstone. 143-147.
- John L.Atlee. Complications in Anaesthesia 2nd Edition Saunders Elsevier 423-425.





