
MBBS, MD (Medicine),
Consultant Physician and Intensivist
Reactive Airways Disease:
Reactive Airways Disease is a general term for conditions involving wheezing and allergic reactions.(1)
Reactive Airways Dysfunction Syndrome (RADS):
RADS is a term proposed by Stuart M Brooks and colleagues in 1985(2) to describe an asthma like syndrome developing after a single exposure to high levels of an irritating vapor , fume or smoke.(3) It involves coughing , wheezing and dysnea.(4)
It can also manifest in adult with exposure to high levels of chlorine , ammonia ,acetic acid or sulphur dioxide creating symptoms like asthma.(5) The severity of these symptoms can be mild to fatal and can create long term airway damage depending upon the amount of exposure and concentration.
Some experts classify RADS as occupational asthma.(6)
RADS mistakenly used as synonym for asthma.(7)
BRONCHIAL ASTHMA
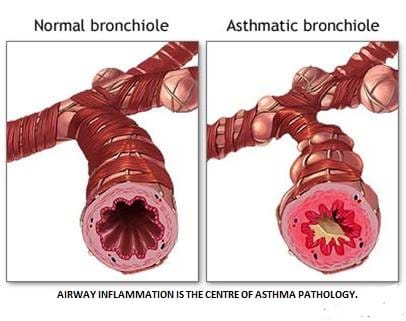
Bronchial Asthma is a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role. The chronic inflammation is associated with airway hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness, and coughing, particularly at night or in the early morning. These episodes are usually associated with widespread, but variable, airflow obstruction within the lung that is often reversible either spontaneously or with treatment.
Magnitude of the Problem in India
There are about 15- 20 million asthmatics in India. A recent study conducted in Delhi established asthma prevalence to be 12% in schoolchildren. It is a significant cause of school/work absence. Health care expenditures are very high. Morbidity and mortality are on rise.
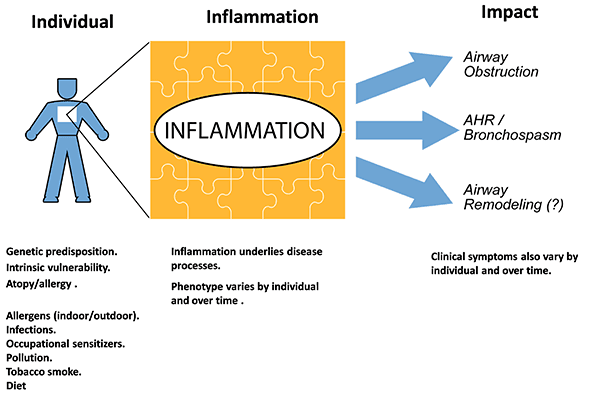
Overview of pathophysiology
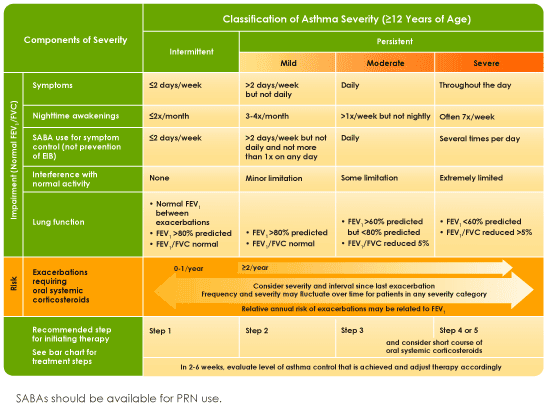
CLASSIFICATION
MANAGEMENT
Principles of Asthma management:
- Identify and avoid asthma triggers
- Control inflammation with Inhaled Corticosteroids (systemic in moderate to severe exacerbations) and other anti-inflammatory agents.
- Relieve bronchospasm with Bronchodilators.a
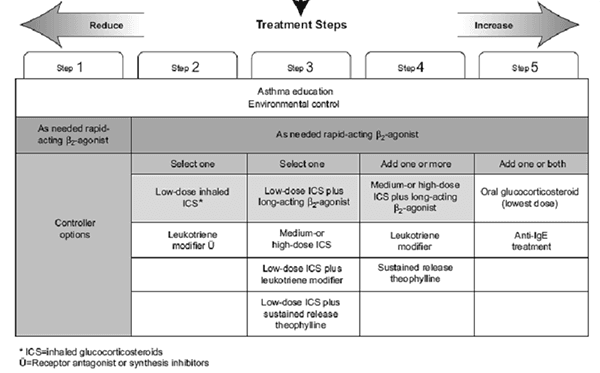
Treatment Steps
Acute Severe Asthma
Severe Exacerbations of asthma is a feared complication and may be life-threatening.
Clinical Features
Patients are aware of increasing chest tightness, wheezing, and dyspnea that are often not or poorly relieved by their usual reliever inhaler. In severe exacerbations patients may be so breathless that they are unable to complete sentences and may become cyanotic. Examination usually shows increased ventilation, hyperinflation, and tachycardia. Pulsus paradoxus may be present, but this is rarely a useful clinical sign. Arterial blood gases on air show hypoxia and PaCO2 is usually low due to hyperventilation. A normal or rising PaCO2 is an indication of impending respiratory failure and requires immediate monitoring and therapy. A chest roentgenogram may show pneumonia or pneumothorax.
Treatment
- A high concentration of oxygen achieve oxygen saturation of >90%.
- High doses of short-acting inhaled beta2-agonists that are given either by nebulizer or via a metered dose inhaler with a spacer
- Systemic corticosteroids.
- In severely ill patients with impending respiratory failure, intravenous beta2-agonists may be given.
- An inhaled anti-cholinergic may be added if there is not a satisfactory response to beta2-agonists alone, as there are additive effects.
- In patients who are refractory to inhaled therapies, a slow infusion of aminophylline may be effective, but it is important to monitor blood levels especially if patients have already been treated with oral theophylline.
- Magnesium sulfate given intravenously or by nebulizer has also been shown to be effective when added to inhaled beta2-agonists, and is relatively well tolerated but is not routinely recommended.
- Prophylactic intubation may be indicated for impending respiratory failure, when the PaCO2 is normal or rises. For patients with respiratory failure, it is necessary to intubate and institute ventilation. These patients may benefit from an anesthetic, such as halothane, if they have not responded to conventional bronchodilators.
- Sedatives should never be given as they may depress ventilation.
- Antibiotics should be used if infection as the cause of exacerbation is identified or suspected..
References:
- ^"Reactive Airway Disease" at Dorland’s Medical Dictionary
- ^ S.M. Brooks, M.A. Weiss, I.L. Bernstein. "Reactive airways dysfunction syndrome (RADS): persistent asthma syndrome after high level irritant exposures". Chest, Volume 88, 1985, 376-384. Retrieved 2007-08-28.
- ^ John V. Fahy and Paul M. O’Byrne. ""Reactive Airways Disease": A Lazy Term of Uncertain Meaning That Should Be Abandoned". Am. J. Respir. Crit. Care Med., Volume 163, Number 4, March 2001, 822-823. Retrieved 2007-04-22.
- ^"reactive airways dysfunction syndrome" at Dorland’s Medical Dictionary
- ^ Aslan, Sahin1Kandiş, Hayati1Akgun, Metin2Çakır, Zeynep1Inandı, Tacettin3Görgüner, Metin (2006). "The Effect of Nebulized NaHCO3 Treatment on ‘RADS’ Due to Chlorine Gas Inhalation". Inhalation Toxicology: Vol. 18, Number 11. ISBN 895-900 Check |isbn= value (help). Retrieved 2008-04-06.
- ^Occupational Allergy. Page 1 Drs Rodney Ehrlich and Mohamed F Jeebhay. The Allergy Society of South Africa
- ^ Mayo Clinic Staff (September 4, 2006). "Reactive airway disease: Is it asthma?". Mayo Clinic. Retrieved 2007-04-22.





