
Professor of Medicine and Director,
Center for Health Professionals Education & Research
Jawaharlal Nehru Medical College, Sawangi (Meghe), Wardha
Fever of unknown origin identifies the syndrome that does not resolve spontaneously where cause remains elusive after an extensive diagnostic workup. The term of Fever of Unknown origin was coined by Petersdorf & Beeson (1961)1 and defined as temperature of more than 38° C on most of the occasions for more than 3 weeks and with a diagnosis that remains uncertain after one week’s extensive investigations. The authors chose three weeks period to exclude the self limiting illnesses like viral fevers and to allow sufficient time for initial investigations for the cause of fever. With modern mechanisms for investigation of cases quickly, this period for investigations can be curtailed. The fever of unknown origin is often frustrating to physician as well to patients because the diagnostic workup often involves numerous invasive and non invasive investigations that sometime fail to explain the cause of fever. In FUO, there is no structured gold standard test for diagnosis of the disease and often varies from case to case.
To have structured, sensible and effective approach, the clinicians should have understanding of the spectrum of disease and the tests characteristic of the various diagnostic modalities available for evaluation of FUO.
What is fever?
The oral temperature of more than 37.2° C, rectal and Tympanic temperature 0.5° higher than oral temperature and axillary temperature lower by 0.5°C is characteristic of Fever. Women have higher normal temperature by 0.2°C while there is no difference in temperature of old or young persons2.
Fever can be short and self-limited where no extensive diagnostic tests or specific therapy is required as in viral infections or upper respiratory tract infections or it can occasionally be a manifestation of serious disease or may be contagious and often quite easy to diagnose and to treat efficiently. Examples of such illness can be bacterial pneumonia, urinary tract infection, erysipelas, sinusitis, cholecystitis, appendicitis & influenza2.
There can be no fever despite infections in newborn babies, elderly, chronic hepatic or renal failure, corticosteroid treatment or bacteremic shock.
Hints at severe febrile illness includes recent travel to tropics particularly where there is malaria, fever with chills, Temperature >39°C, continuous Fever with a rash, extremes of age, any known or suspected immuno suppression and neurological signs and symptoms.
Effects of Fever:
Fever has beneficial effects like immune-stimulation (macrophages, lymphocytes stimulation) through temperature sensitive organisms and also has Harmful effects like increased O2-consumption, increased circulation, catabolism, fluid loss and enzymatic functions with temperature more than 41°C.
Etiology of FUO 3
- Classic PUO: Includes subtypes like
Infectious: Abscess, Endocarditis, Tuberculosis, Complicated UTI
Connective tissue diseases: SLE, Rhumatoid Arthritis, Stills Disease, Polymyalgia Rheumatica, Temporal arteritis
Neoplastic: Lymphomas, Leukemia or Miscellaneous disorders-alcoholic Hepatitis, granulomatous disorders - Nosocomial: Health care acquired infections.
surgery, use of urinary catheter, intravascular devices , drugs (antibiotics), Drug fever, immobilization sinusitis, nasogastric and orotracheal tubes, Deep Vein Thrombosis, Pulmonary Embolism, Transfusion - Immunodeficient: patients receiving Chemotherapy or in hematologic malignancies.
Fever can be Neutropenic (PNL <500/uL) or because of impaired cell-mediated immunity. - HIV Associated.
Case History
A 33 years old woman was admitted with history of fever and malaise of 5 weeks duration. On physical examination she was febrile with temperature of 39° C, pulse rate of 104 bpm, Blood pressure of 150/50 mmHg. Cardiac examination showed early diastolic murmur at base of heart, bilateral fine basal crepts and had signs of right sided hemiplegia.
Urine examination showed RBC 5-6/hpf, ESR was 120 at end of first hour, ECG showed LVH and X-rays showed cardiomegaly. Total & differential counts were normal, blood for paracheck was negative and all other investigations to find out cause of fever were inconclusive.
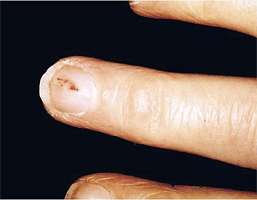
On eighth day after she developed small hemorrhagic spots on skin of upper extremity. Coagulation profile and platelet counts were normal. The detail examination showed small hemorrhagic spot on middle finger.
In view of the early diastolic murmur and fever a possibility of infective endocarditis was considered. The repeat 2-D Echo showed a pedunculated mass on aortic valve. Blood culture was done and one of the samples showed growth of Streptococci viridians. Patient was put on high dose of penicillin and responded on fifth day of therapy.
In this case the only diagnostic clue was small hemorrhagic spots on skin and development of Splinter hemorrhage on nail in a case of aortic incompetence.
CLASSIC FUO:
‘‘Classic’’ FUOs may be defined as disorders with temperatures greater than or equal to 101° F that persists for at least 3 weeks and that is not diagnosed after a week of intensive in-hospital testing.
Most patients of classic FUO have sub acute or chronic symptoms with duration of fever before diagnosis approximately 20-25 days. Temperature of more than 101.0° F (2).
Causes of Classic FUO (3), (4)
Infections
- Tuberculosis
- Abscess – abdomen, pelvic, Dental
- Endocarditis
- Osteomyelitis
- Sinusitis
- Viral infections
- Lyme disease
Malignancies
- Leukemia, Lymphoma, Secondary Metastasis, 1°malignancies.
- Myelodysplastic disorders
Auto immune disorders
- Adult Still’s disease
- Polymyalgia rheumatica
- Temporal arteritis
- Rheumatoid arthritis
- Rheumatoid fever
- Inflammatory bowel disease
- Reiter’s syndrome
- Systemic lupus Erythmatosus
- Vasculitides
Rare miscellaneous causes of Classic FUO
- Alcoholic hepatitis
- Cirrhotic fever
- Granulomatous hepatitis
- Pancreatitis
- Aortic dissection
- Vitamin B12-deficiency
- Pulmonary emboli
- Sarcoidosis
Malignancies cause fever by
- Production and release of pyrogenic cytokines: lymphomas
- Spontaneous or induced tumor necrosis
- Induction of secondary infections: pneumonia
Final diagnosis of Classic FUO
| Diagnosis | Diagnosis | Diagnosis >65years (n=201) |
| Infections | 33 (21%) | 75 (35%) |
| Abscess | 6 | 25 |
| Endocarditis | 2 | 14 |
| Tuberculosis | 4 | 20 |
| Viral infections | 8 | 1 |
| Others | 13 | 12 |
| Tumors | 8 (5%) | 37 (19%) |
| Multisystem diseases | 27(17%) | 57 (28%) |
| Miscellaneous | 39 (26%) | 17 (8%) |
Nosocomial FUO
It is characterized by fever of more than 38.0°C and evidence of some manipulation in hospital setting. The duration of fever is usually less than that of classical PUO.
The common risk factors for nosocomial FUO includes surgery, instrumentation to urinary or respiratory tract, intravascular devices, drug therapy, and immobilization Common examples are –
- Septic thrombophlebitis,
- Recurrent pulmonary emboli
- Clostridium difficile colitis,
- Intracranial mass effects following stroke
- Ventilator-associated Pneumonia
- Drug induced
Common drugs that cause FUO are (4)
| Allopurinol | Captopril |
| Cimetidine | Clofibrate |
| Erythromycin | Heparin |
| Hydralazine | Hydrochlorthiazide |
| Nifidepine | Methyldopa |
| Nitrofurantoin | Penicillin |
| Phenytoin | Procainamide |
| Quinidine | Isoniazid |
Immunodeficient FUO
It is also known as neutropenic FUO.
It is defined as recurrent fever in a patient whose neutrophil count is 500 per mm3 or less
It can be assessed for three days without establishing an etiology for the fever.
In most of these cases, the fever is caused by opportunistic bacterial infections.
These patients are usually treated with broad-spectrum antibiotics to cover the most likely pathogens. Occult infections caused by fungi, such as hepatosplenic candidiasis and aspergillosis, herpes simplex virus infections. The characteristic skin findings may be present in some cases.
Case History
A 62-year-old female was admitted to the hospital with haemoptysis, polyarthralgia, fever, weight loss, night sweats. One month prior to the admission she had reported the nose pain, rhinorrhea and epistaxis, and she received nonspecific antibiotic therapy, without any improvement. She denied smoking and alcohol use. At the time of hospital admission, the patient was conscious; her body temperature was 37.5°C, pulse 130/min, respiration rate 20/min, and blood pressure 90/60 mmHg. She was adynamic, pale, upset, with haemoptysis. Her nostrils and throat were erythematous, with coagulum on the right nostril. On her tongue, palate and buccal mucosa there were diffuse aphtous ulcerations. Her neck was supple, with no meningeal signs. Bilateral basal rales were observed on the lung auscultation.
Normal cardiac auscultation was reported. Her abdomen was neither tender nor distended, there were no edema, cyanosis or clubbing of the extremities.
Laboratory investigations showed WBC 18,4 x 104/μl, RBC 3,92×106/μl, hemoglobin 8,6 g/dL, Platelets 902x 103/μl, ESR 110 mm/h
Biochemical parameters
CRP 252,2 mg/dl, glucose 4,7 mmol/l, urea 9,8 mmol/l, creatinine 135 μmol/l, alkaline phosphatase 155 U/l, AST 39 U/l, ALT 65 U/l, LDH 702 U/l, protein 64 g/l, albumin 29 g/l, Calcium 2,19 mmol/l, Sodium l40 mmol/l, Chloride 98 mmol/L
Urine analysis- hemoglobin +, albumin +, sediment Lot of red blood cells casts.
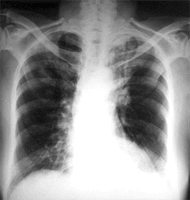
Chest CT scan showed two infiltrates in the right upper lobe, (33×24 mm and 20×19 mm) and consolidation on the left upper lobe.
CT scan showed mucosal thickening in the right maxillary sinus, and nasal septum deviation.
Sputum culture showed Streptococcus pneumonia. Ziehl-Neelsen stain and culture for acid fast
Bacilli were negative. Urine culture showed providentia on mass. Chemo-culture was sterile.
Results of the test for human immunodeficiency (HIV) virus were negative. Sputum cytology showed a lot of red blood cells and polymorphonuclear cells. Hematological examination showed leukocytosis and hypochromic anemia. Ultra-sonography of the abdomen showed the splenomegaly (125×82 mm), and Flexibile fiber optic bronchoscopy revealed mucosal erythema and edema suspected to have malignancy.
Patient was put on therapeutic trial of anti-tubercular drugs. In spite of the therapy, the patient had hemoptysis. Radiological finding was unchanged. At day 17, the patient developed palpable purpura
on the lower extremities. Dermatologist was consulted, .and suspected of purpura Hoenoch Shoenlain.
Immunological parameters showed Negative Antinuclear antibodies, IgG 18.81g/l, IgM 1.24 g/l IgA 4.47 g/l C3 1,54 g/l, cANCA 24 U/ml, pANCA 9 U/ml.
Antitubercular drugs were discontinued and patient was put on Prednisolone considering a possibility of Wegner’s Granulomatosis (5).
WG is classified as ANCA positive vasculitis, mostly localized on the small and medium-sized blood vessel. It mostly affects the upper and lower respiratory airways and kidneys.
HIV associated fever – Characterized by (4)
Temperature >38.3°C
Duration of > 4 weeks for outpatients, >3 days for inpatients
HIV infection confirmed
Common Etiologies of fever in HIV associated fever are Cytomegalovirus, Mycobacterium avium-intracellulare complex, Pneumocystis carinii pneumonia, drug-induced, Kaposi’s sarcoma and lymphoma.
Case History
A 50 yrs male was admitted for CABG. Pt underwent the opration without complications. All inv including HIV were negative.
Patient developed fever 3 weeks after operation. All investigations to find out the cause of fever were negative. CBC showed Hb 8 Gm %, TLC 3000/cmm, L- 50% All Investigations like KFT, LFT, CXR, USG abdomen , MRI Brain & ANCA were Negative. Urine NAD CXR did not show any shadows in lung.
Review history of patient was taken. It was inconclusive except the history of travel to USA 1 month prior to admission to hospital for operation. In view of this history repeat ELISA for HIV and CD 4 cell count was done. Blood was positive for HIV 1 & HIV 2 and CD4 count was 100 cells/ mm3. The Sputum showed PCP . Patient was put on ART and Septran. His fever disappeared after 10 days.
Factitious Fever (2)
Patients manipulate thermometers & temperature record. Factitious fever is responsible for 10% of FUO cases. It is most commonly seen in young adults with healthcare experience or knowledge. Evidence of psychiatric problems or a history of multiple hospitalizations is common.
Rapid changes of body temperature without associated shivering or sweating, large differences between rectal and oral temperature and discrepancies between fever, pulse rate, or general appearance are observed.
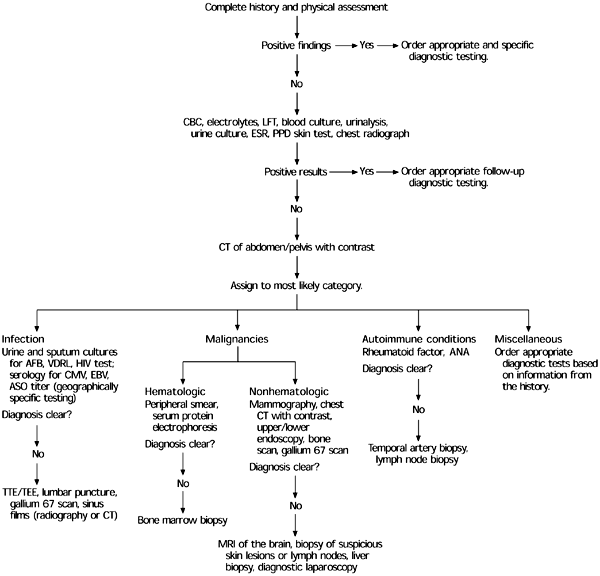
Evaluation of the Patient with FUO (4)
The initial approach to the patient presenting with fever should include a comprehensive history, physical examination, and appropriate laboratory testing. As the underlying process develops, the history and physical assessment should be repeated. The first step should be to confirm a history of fever and document the fever pattern. Classic fever patterns such as intermittent, relapsing sustained, and temperature-pulse disparity may prove to be useful but rarely are diagnostic.
In taking a history from a patient with FUO, particular attention should be given to recent travel, exposure to pets and other animals, the work environment, and recent contact with persons exhibiting similar symptoms. In patients returning from areas where tuberculosis and malaria are common, the index of suspicion for these diseases should be elevated. In patients who have had contact with pets or other animals, diseases common to animal handlers must be suspected.
The medical history also must be examined for conditions such as lymphoma, rheumatic fever, or a previous abdominal disorder (e.g., inflammatory bowel disease), the reactivation of which might account for the fever. Finally, drug-induced fever must be considered in patients who are taking medications.
Diagnostic significance of fever patterns
Morning temperature spikes (6)
In obscure causes of FUO, fever curves are useful diagnostically and often provide the only clue to the diagnosis. The first step in evaluating fever patterns is to determine the time of the peak period during a 24-hour period. Most patients with fever have peak temperatures in the late afternoon or early evening. This means that there are relatively few disorders associated with morning temperature elevations. If not altered by antipyretic medications or devices, the periodicity of fever can be a useful diagnostic aid in obscure cases of FUO. The causes of FUO associated with morning temperature elevations are typhoid fever; tuberculosis; and among the noninfectious disorders, periarteritis nodosa.
Relative bradycardia (6)
A pulse-temperature deficit is termed ‘‘relative bradycardia’’ (Faget’s sign). For a pulse temperature to be termed relative bradycardia there must be a significant pulse temperature deficit relative to the degree of fever. Relative bradycardia should not be applied to children or those with temperatures of less than 102° F or adults with temperatures of less than 102° F or those on b-blockers, diltiazem, verapamil, or who have pacemaker-induced rhythms or arrhythmias. The pulse rate for any given degree of temperature elevation is physiologic and predictable. For every degree of temperature elevation in degrees Fahrenheit there is a concomitant increase in pulse rate of 10 beats per minute. In the absence of the exclusion criteria mentioned, a temperature of 104° F should be accompanied by an appropriate pulse response of 130 beats per minute. This patient with relative bradycardia would have a pulse less than or equal to 120 beats per minute. Applied correctly relative bradycardia is an important diagnostic sign. In FUO patients, relative bradycardia may occur in association with malaria, typhoid fever, any central nervous system disorder, some lymphomas, and drug fever.
Relative tachycardia refers to an inappropriately rapid pulse for a given degree of temperature, and is only associated with pulmonary emboli among the causes of FUO.
Double quotidian fevers (7)
Double quotidian fevers refer to two temperature spikes occurring within 24-hour period. Although double quotidian fevers are not a common fever pattern, they are most helpful when present in febrile patients presenting with a differential diagnosis. Infectious causes of FUO associated with double quotidian fevers include miliary tuberculosis, visceral leishmaniasis, and mixed malarial infections. In returning travelers from India, malaria and typhoid fever are important differential diagnostic considerations.
Camelback (dromedary) fevers (6)
A camelback or dromedary fever curve is one that has a few days with fever, separated by a decrease in fever between the febrile episodes over the period of a week. Graphed on temperature chart the two periods of temperature prominence are separated by a period of decreased temperatures, resembling a two-humped camel or dromedary silhouette. As with other unusual fever curves, camelback fever patterns are of most use when the differential diagnosis includes obscure otherwise difficult-to-diagnose infections.
Presenting as FUOs. A camelback fever curve may occur in leptospirosis, brucellosis, and ehrlichiosis.
Relapsing fevers (7)
Relapsing fevers refer to those that are recurring and separated by periods with low-grade fever or no fever. Rat-bite fever, relapsing fever, Bartonella, tuberculosis, and relapsing fever patterns are important in FUOs because, by definition, the fever in patients with FUOs is of long duration (ie, R3 weeks). Inherent in the definition of a relapsing fever is the notion that the underlying disorder responsible for ongoing fever continues to be clinically active in terms of its febrile expression. In contrast, recurrent fevers recur.
Periodically and are associated with fever flares, which is an expression of the flare of the underlying disorder (eg, SLE). A relapsing fever pattern may be difficult to appreciate in acute fevers where the duration of the fever may not permit an appreciation of the relapsing nature of the fever. Among the infectious causes of FUO, relapsing fever pattern is classically associated with relapsing fever (Borrelia recurrentis) but has also been associated with typhoid fever, malaria, brucellosis, and rat-bite fever.
Nonrelapsing fevers may also be caused by a variety of noninfectious etiologies. In the FUO patient, noninfectious causes of relapsing fever include cyclic neutropenia, familial Mediterranean fever, SLE, vasculitis, hyperimmunoglobulinemia D syndrome, and Schnitzler’s syndrome. Relapsing fevers may be Mimicked by antipyretic interventions, and by inappropriately or partially treated infectious diseases in FUO patients.
Diagnostic clues often are not readily apparent on physical examination; repeated examination may be essential. Careful attention to the skin, mucous membranes, and lymphatic system, as well as abdominal palpation for masses or organomegaly, is important. The physician’s choice of imaging should be guided by findings from a thorough history and physical examination (e.g., a cardiac murmur in the presence of negative blood cultures should be investigated with a transthoracic echocardiogram or, if needed, transesophageal echocardiogram) Duke’s clinical criteria include two major and six minor criteria that help determine the likelihood of endocarditis.
Diagnosis of Fever of Unknown Origin (4)
A chest radiograph also should be obtained in all patients to screen for possible infection, collagen vascular disease, or malignancy. If this initial assessment does not disclose the source of fever, more specific investigatory techniques, such as serology, sonography, computed tomography (CT), magnetic resonance imaging (MRI), and nuclear medicine scanning should be conducted, based on clinical suspicion.
Abdominal sonography, pelvic sonography, or CT scanning should be performed early in the diagnostic process to rule out such common causes of FUO as intra-abdominal abscess or malignancy, depending on the primary evaluation. This testing, including directed biopsies, has greatly reduced the need for more invasive operative studies.
MRI should be reserved for clarifying conditions found through the use of other techniques or when the diagnosis remains obscure. The use of radionucleotide scanning, such as gallium 67, technetium Tc 99m, or indium-labeled leukocytes, is warranted for detecting inflammatory conditions and neoplastic lesions that often are underdiagnosed by CT scans; however, these tests tend not to detect collagen vascular disease and other miscellaneous conditions.
Diagnostic usefulness of the Naprosyn test (7)
The Naprosyn test was first developed by Chang, an oncologist. Using Naprosyn (naproxen) over a 3-day period (375 mg orally twice daily) he was able to differentiate neoplastic from infectious FUOs. The Naprosyn test is considered positive when there is a rapid or sustained defervescence during the 3 days of the test period. Fever in patients with neoplastic disorders recurs after cessation of the Naprosyn test. Those with infectious diseases undergo little or no drop in their temperatures during the test period.
Diagnostic Imaging in Patients with FUO (9), (10)
| Imaging | Possible diagnoses |
| Chest radiograph | Tuberculosis, malignancy, Pneumocystis carinii pneumonia |
| CT of abdomen or pelvis with contrast agent | Abscess, malignancy |
Gallium 67 scan | Infection, malignancy |
Indium-labeled leukocytes | Occult septicemia |
Technetium Tc 99m | Acute infection and inflammation of bones and soft tissue |
| MRI of brain | Malignancy, autoimmune conditions |
| PET scan | Malignancy, inflammation |
| Transthoracic or transesophageal echocardiography | Bacterial endocarditis |
| Venous Doppler study | Venous thrombosis |
Invasive diagnostic tests
Liver biopsy (11)
If there are signs and symptoms in a presenting FUO syndrome complex that suggest liver involvement, then liver biopsy may be diagnostically helpful. Liver biopsy is most useful in granulomatous hepatitis where the differential diagnosis may be useful in differentiating granulomas caused by infections,
Rheumatic-inflammatory disorders, or neoplastic causes. A liver biopsy may be useful in diagnosing suspected miliary tuberculosis as a cause of FUO.
Lymph node biopsy (12), (13)
Lymph node biopsy is most useful to diagnose lymphomas. Anterior cervical, axillary, or inguinal nodes should not be biopsied if at all possible because the pathology is invariably reported as ‘nonspecific/reactive cannot rule out lymphoma.’’ The preferred nodes to biopsy are the posterior cervical,
epitrochlear, or supraclavicular nodes. Lymph node pathology is diagnostic with lymphoma, ymphogranuloma venereum, toxoplasmosis, and Kikuchi’s arteritis. Granulomas in lymph node biopsies may represent a granulomatous disorder (eg, tuberculosis, sarcoidosis) and lymphoma Bone marrow biopsy
Bone marrow biopsy (14), (15)
As with liver biopsy, may be helpful diagnostically with disorders that are associated with bone marrow abnormalities. Bone marrow biopsy is of importance in diagnosing various neoplastic disorders.
Bone marrow biopsy is also useful diagnostically in cases of suspected miliary tuberculosis.
Bone marrow biopsy is also helpful in a variety of miscellaneous disorders not usually associated with abnormal bone marrow findings (eg, temporal arteritis).
Exploratory laparotomy
Exploratory laparotomy is useful primarily to obtain lymph node or organ biopsies that are otherwise unobtainable. Blind exploratory laparotomy has a low diagnostic yield. The clinical syndromic presentation and the pattern of physical and laboratory abnormalities determines the pattern of organ involvement, which should guide the surgeon to the appropriate tissue when doing an exploratory laparotomy.
Therapy of FUO (16)
The empiric treatments, particularly in the early stages of evaluation, is not recommended.
Continued observation and evaluation while searching for the underlying cause is thought to be the best strategy. Additionally, it is important to withhold therapy until the cause of the fever has been determined, so it can be tailored to a specific diagnosis. Most studies recommend empiric therapy for FUO in only four situations:
- Antibiotics for culture-negative endocarditis
- Low-dose corticosteroids for presumed temporal arteritis
- Antituberculosis drugs for suspected miliary tuberculosis
- Naproxen for suspected neoplastic fever.
It is commonly accepted that diagnosis-defying cases of FUO carry favorable prognoses. Often, empiric therapy may only partially treat a process, making it difficult or impossible to determine subsequent optimal therapy by obscuring an actual diagnosis.
Specific Therapy (3)
Specific therapy includes anti tubercular therapy, anti neoplastic therapy, corticosteroids therapy antibiotics depending upon the final diagnosis in a case of FUO.
Summary
FUOs are caused by variety of causes. These can infections, Collagen vascular diseases, HIV infections or immune-compromization.. FUO usually are limited by their progression and are self-terminating or are terminated with effective therapy. Some causes of FUO are prone to recurrence. Recurrent FUOs are most often caused by rheumatic & inflammatory etiologies.
Patients with infectious FUOs usually resolve with or without therapy in less than a year. Neoplastic disorders usually present themselves in less than 1 year but some disorders may recur episodically over a prolonged period of time The diagnosis of FUO can be done in most cases by various investigations. The non invasive as well as invasive investigations are done based on the need. The treatment is based on the cause of FUO.
References
- Petersdorf RG, Beeson PB. Fever of unexplained origin.Medicine (Baltimore)1961;40:1-30.
- Stefan Zimmerli: Institutfür Infektion skrankheiten: Universität Bern/Inselspital Friedbühlstrasse Fever –fever of unknown: Http://www.ifik.unibe.ch/de/index/weiterbildung/vortraege.php
- Jefrey A,Michel V. Callahan: Fever of Unknown origin:Harrison’s Principles of Internal Medicine:17th Edition, vol. 1, 130-134
- ALAN R. ROTH, D.O., and GINA M. BASELLO, D.O Approach to the Adult Patient with Fever of Unknown Origin: Am Fam Physician. 2003 Dec 1;68(11):2223-2229.
- Tatjana Radjenovic Petkovic, Milan Radovic, Tatjana Pejcic, Milan Rancic, Desa Nastasijevic Borovac and Ivanka Djordjevic: Wegener’s Granulomatosis- case report: Acta Medica Medianae 2008,Vol.47: 78-80
- Cunha BA. The diagnostic significance of fever curves. Infect Dis Clin North Am 1996;10: 33–44
- Cunha BA. Diagnostic significance of relative bradycardia. Infectious Disease Practice 1997; 21:38–40.
- Burke A. Cunha, MD, MACP: Fever of Unknown Origin: Focused Diagnostic Approach Based on Clinical Clues from the History, Physical Examination, and Laboratory Tests: Infect Dis Clin N Am 21 (2007) 1137–1187.
- Knockaert DC, Vanneste LJ, Vannester SB, et al. Fever of unknown origin in the 1980s: an update of the diagnostic spectrum. Arch Intern Med 1992; 152:51–5.
- Gorbach SL, Bartlett JG, Blacklow NE, editors. Infectious diseases. 3rd edition. Philadelphia: Lippincott Williams & Wilkins; 2005.
- Ophyr & Valerie Palda: A comprehensive evidence based approach to FUO: Arch. Of Int. Medicine: 2003:163: 545-551.
- Purnendu S, Louria DB. Non-invasive and invasive diagnostic procedures and laboratory methods. In: Henry W Murray, editor. FUO of undetermined origin. Mount Kisco (NY): Futura Publishing Company; 1983.
- Holtz T, Moseley RH, Scheiman JM. Liver biopsy in fever of unknown origin: a reappraisal. J Clin Gastroenterol 1993;17 :29–32.
- Sinclair S, Beckman E, Ellman L. Biopsy of enlarged superficial lymph nodes. JAMA 1974; 228:602–3.
- Tanaka PY, Hadad DJ, Barletti SC, et al. Bone marrow biopsy in the diagnoses of infectious and non-infectious causes in patients with advanced HIV infection. J Infect 2007;54: 362–6.
- Ka-Yan Chan and Ka-Wing Lee: Pyrexia of unknown origin: Bulletin on The Rheumatic Diseases in Hong Kong: 2001: Vol 1, $0-44





